Category: BPD/DS
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
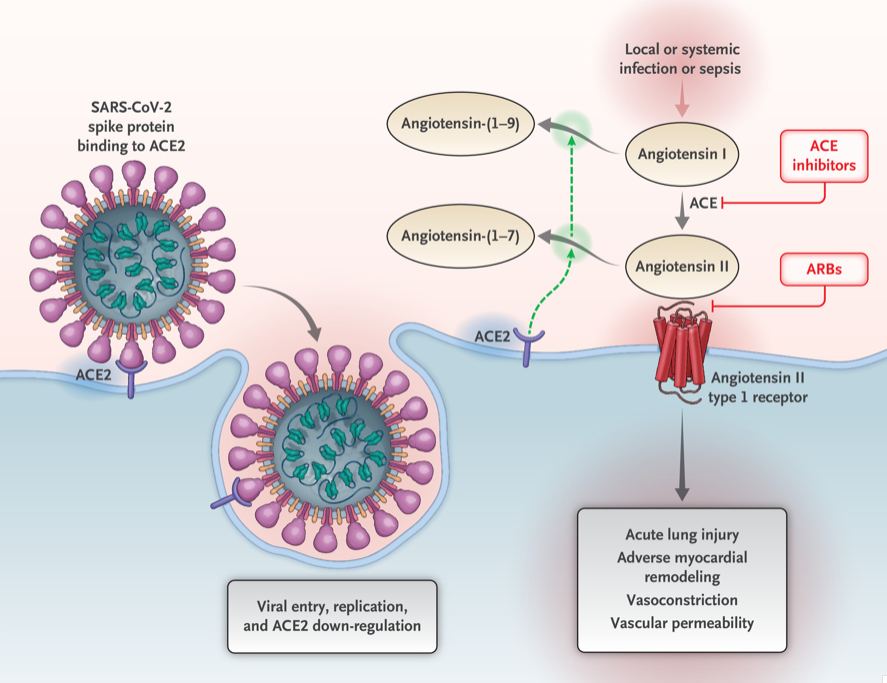
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
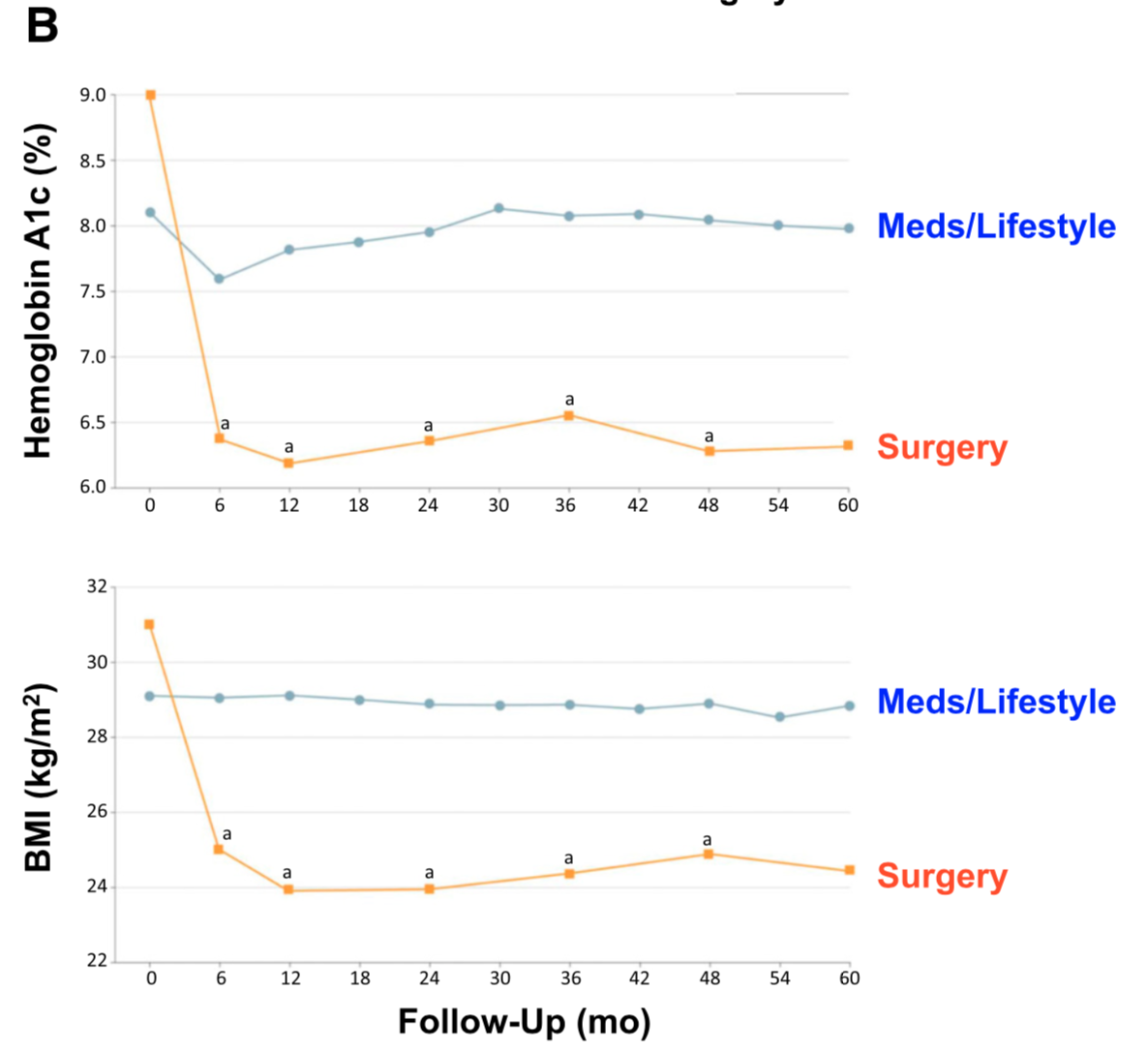
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.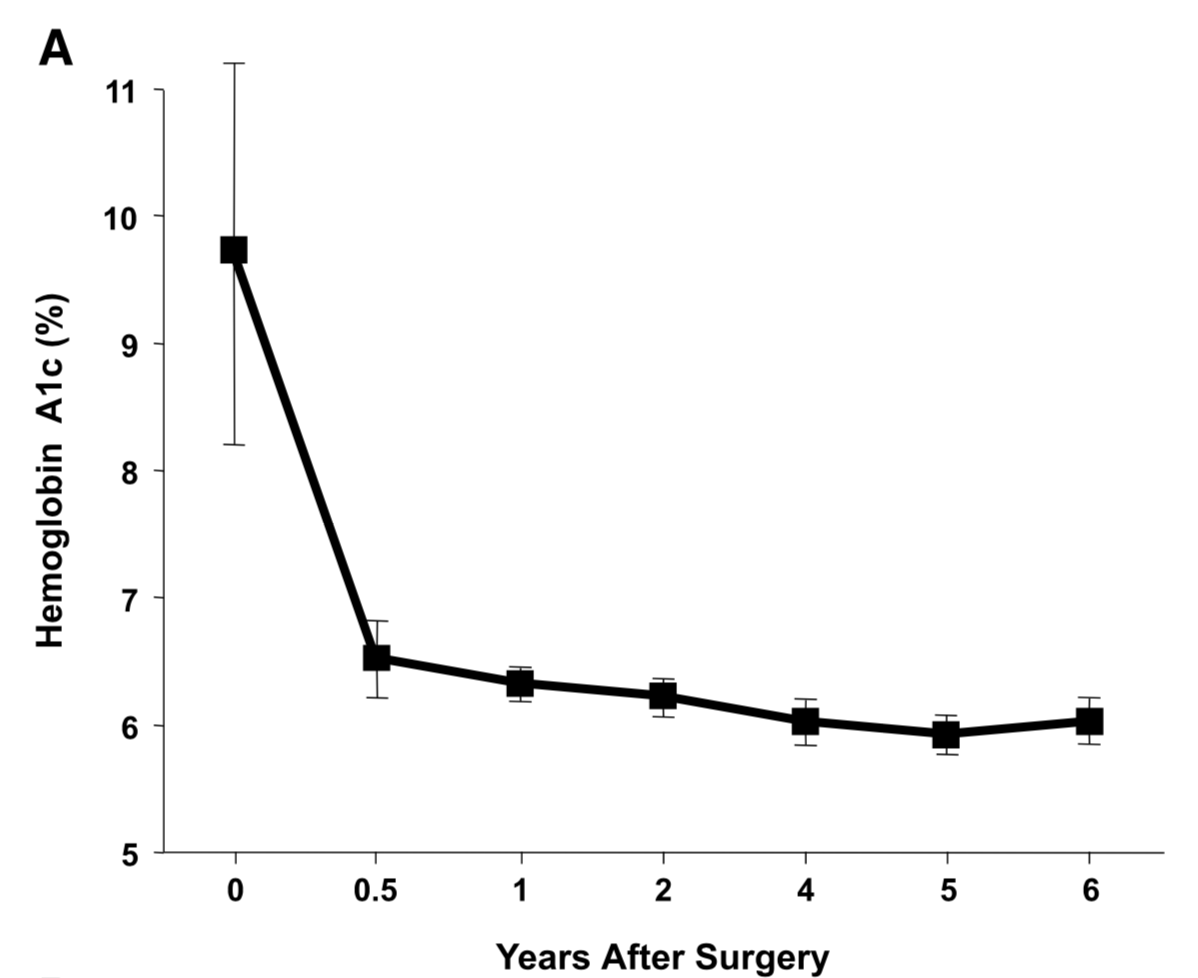
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
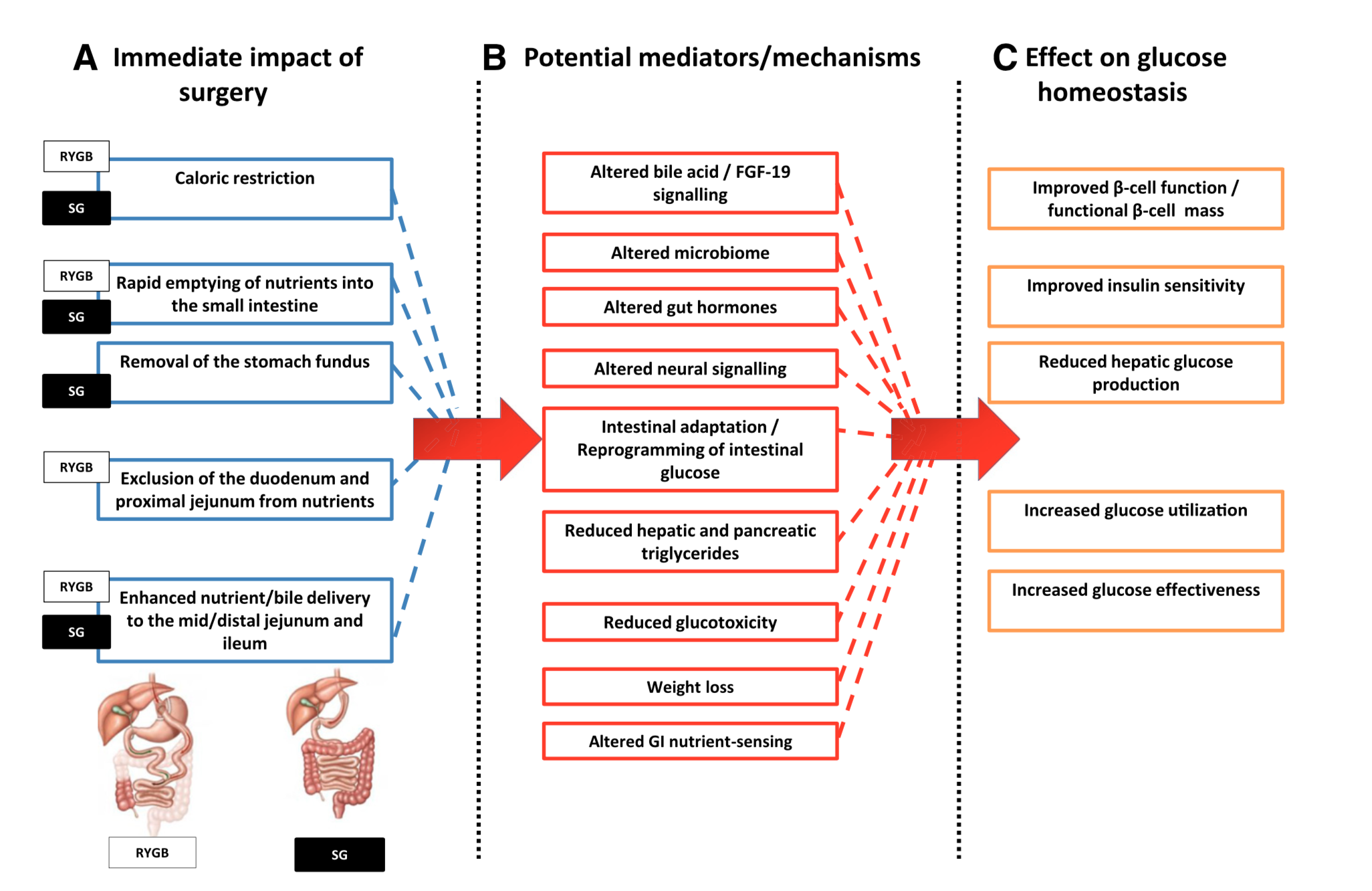
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Osteoporosis Medications
March 28, 2020 7:22 pm
There are a number of lectures, posting that we have done over the years on this topic. However the questions of osteoporosis medications and their benefits and risks comes up often.
The links are attached:
Here is an updated list of medication that I had previously published. I made some clarification to explain how the medications work. There are different classes of medications and the detail of the action and soda effects were described earlier at a blog post.
List of medications that effect bone health.
The table is obtained from https://www.nof.org site.
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Articles
March 22, 2020 6:57 pm
Stapled Anastomosis
December 30, 2019 11:23 am
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
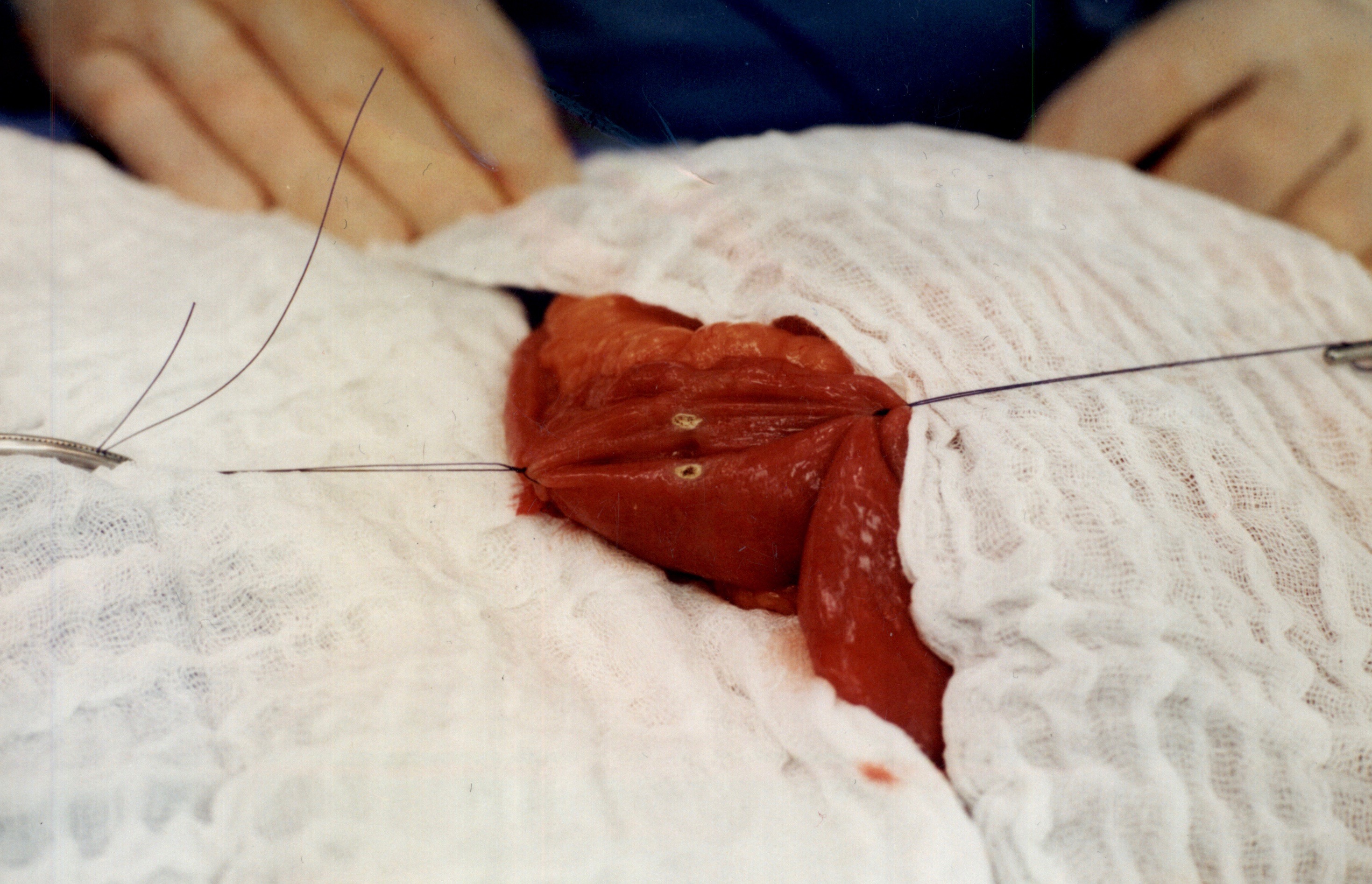
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
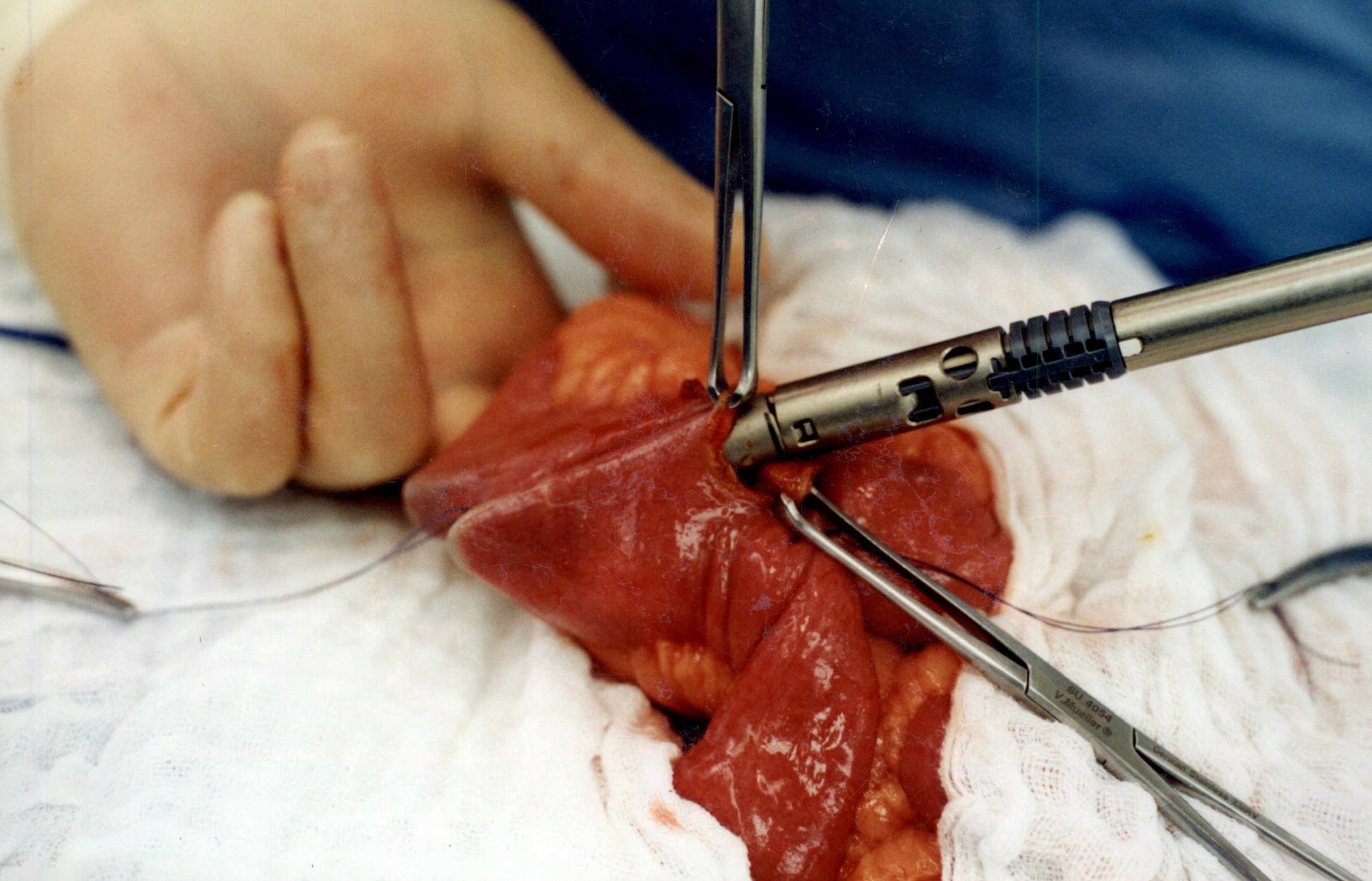
When the stapler is fired in opposite direction, a very wide anastomosis is created.
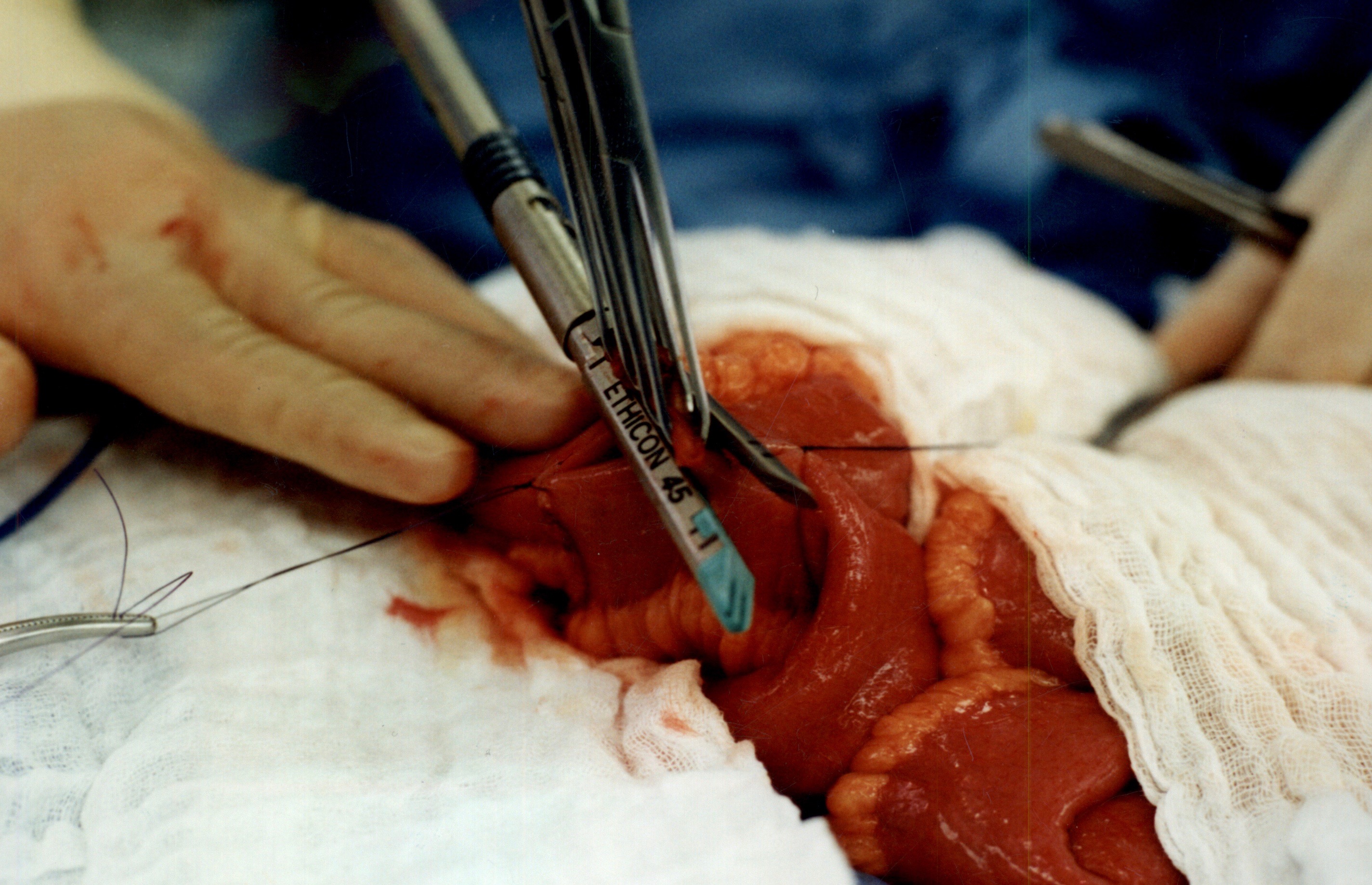
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
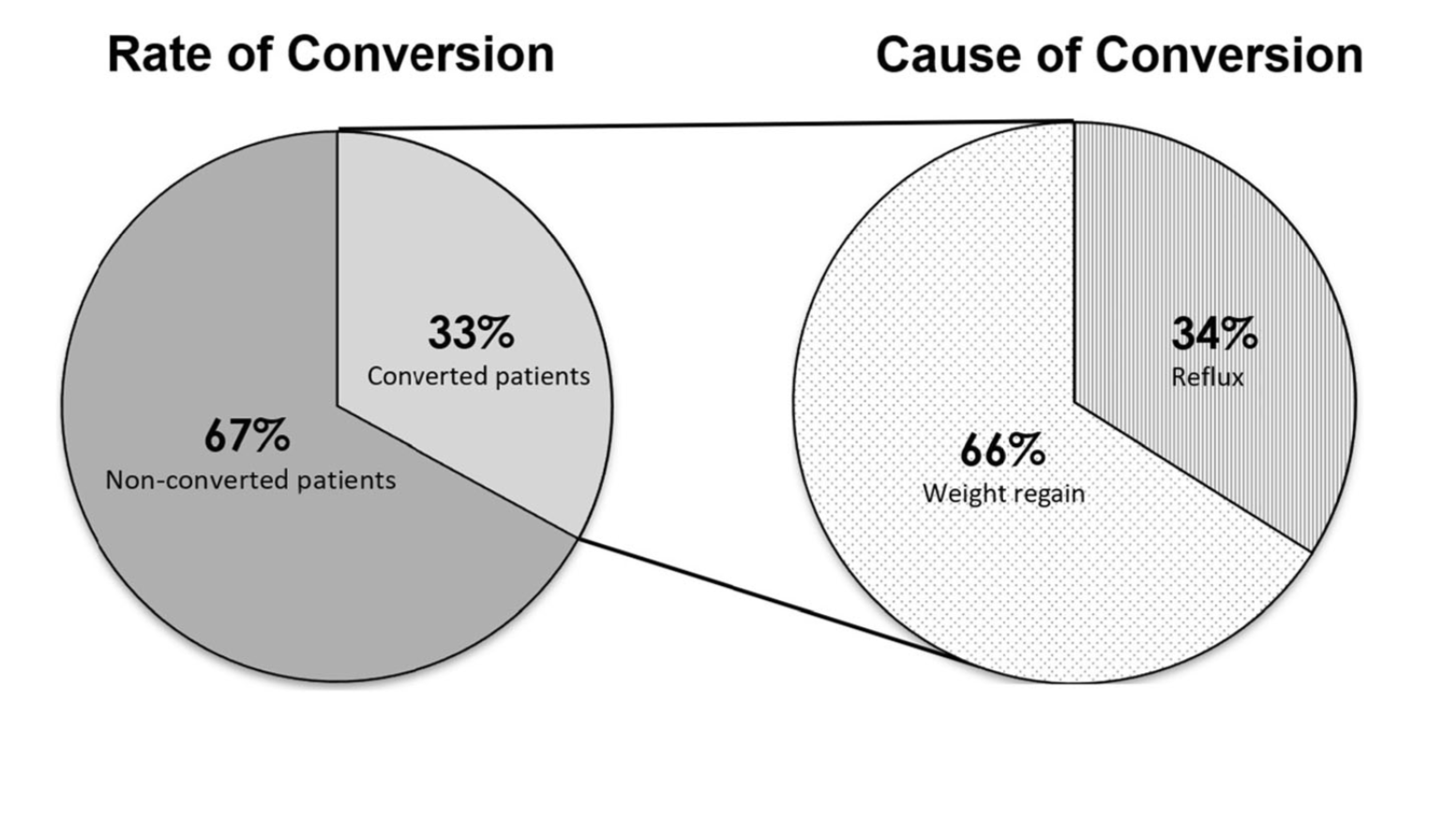
Sleeve And Weight Regain
July 22, 2019 9:50 am
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”