Tag: GRDS
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
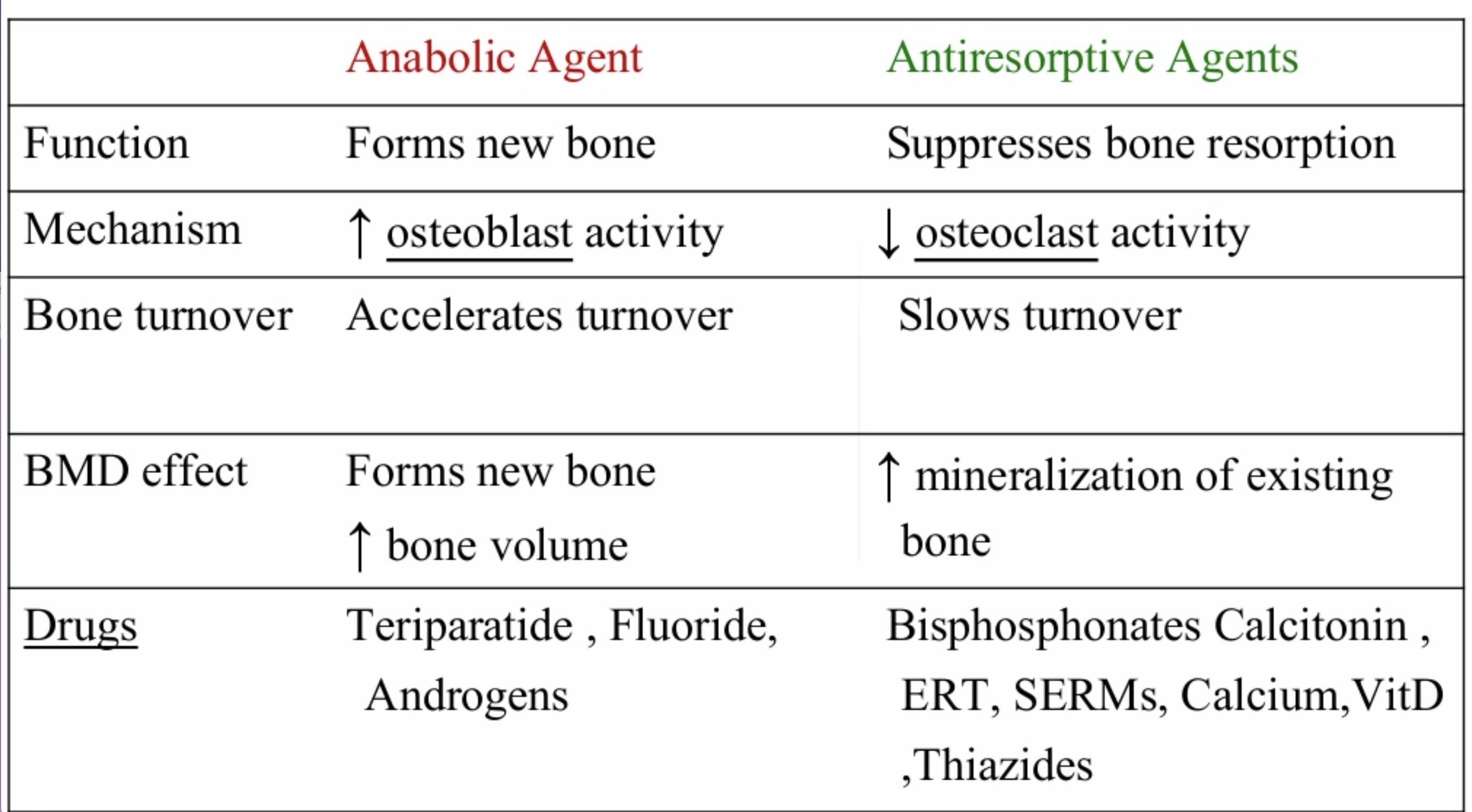
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
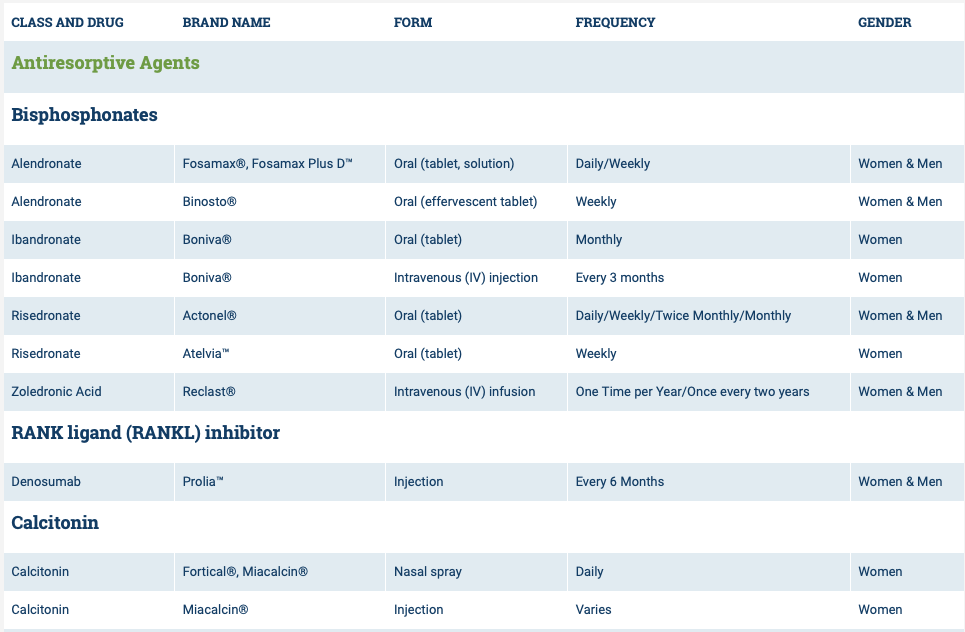
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.

The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
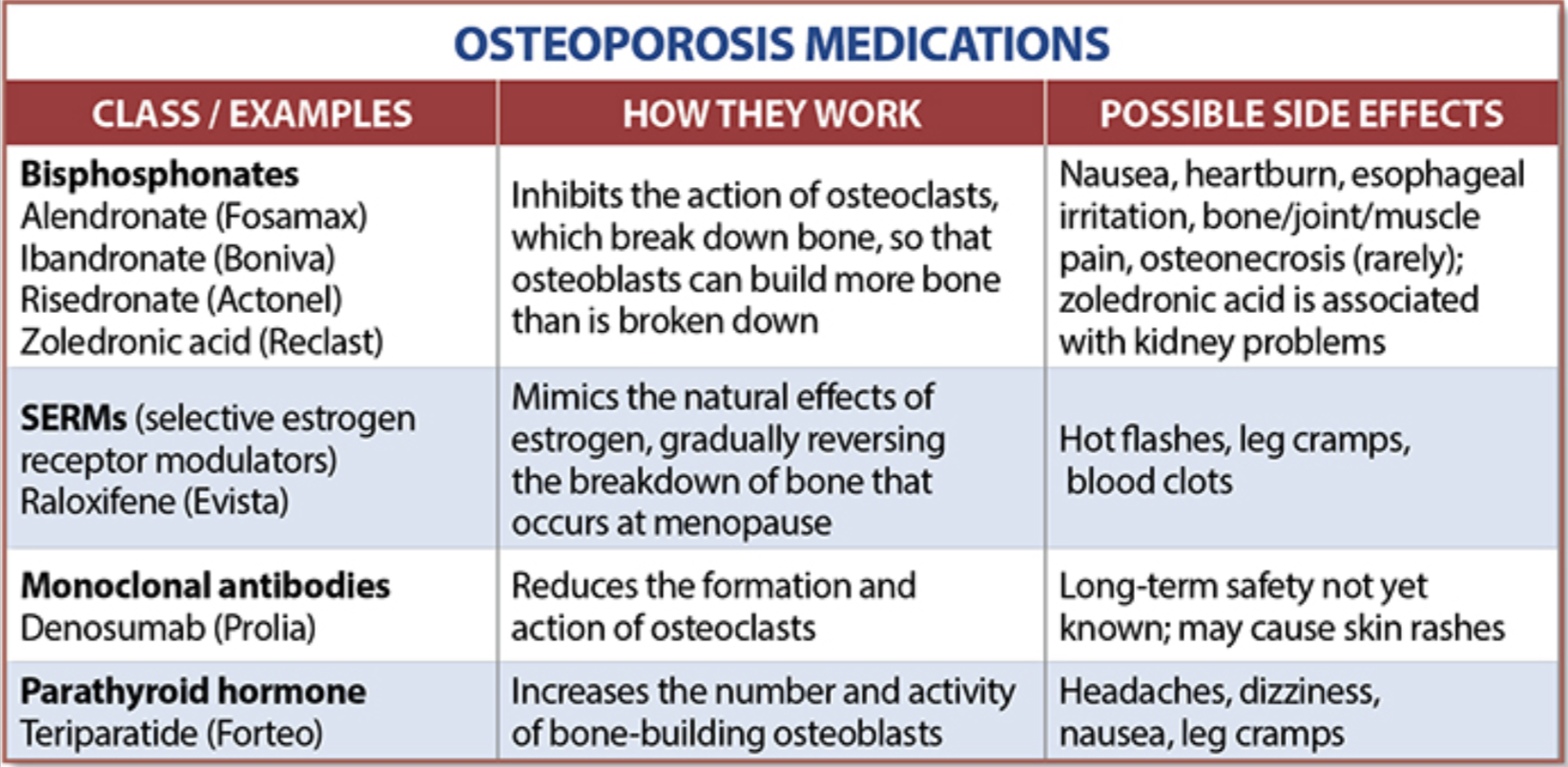
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
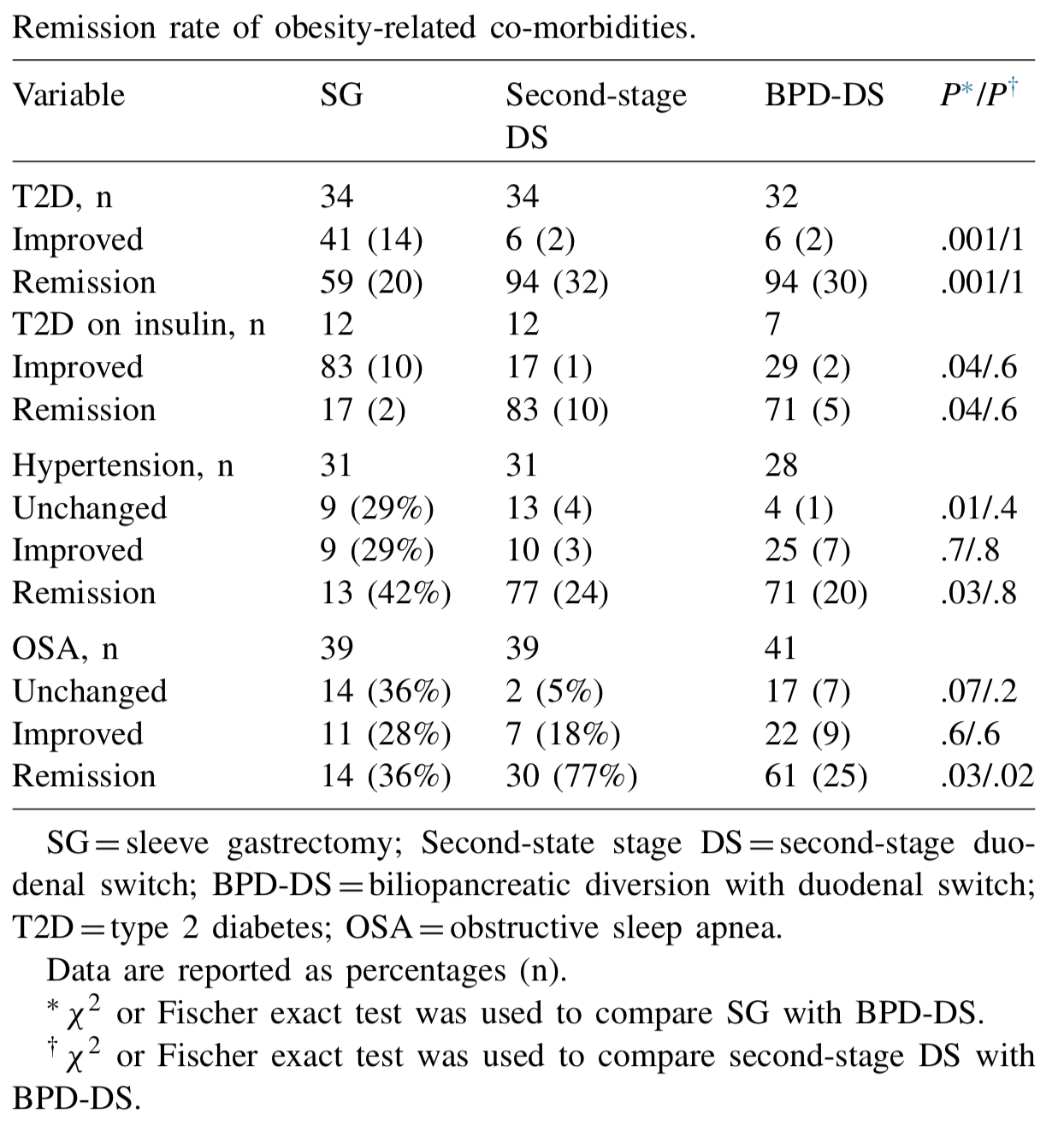
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 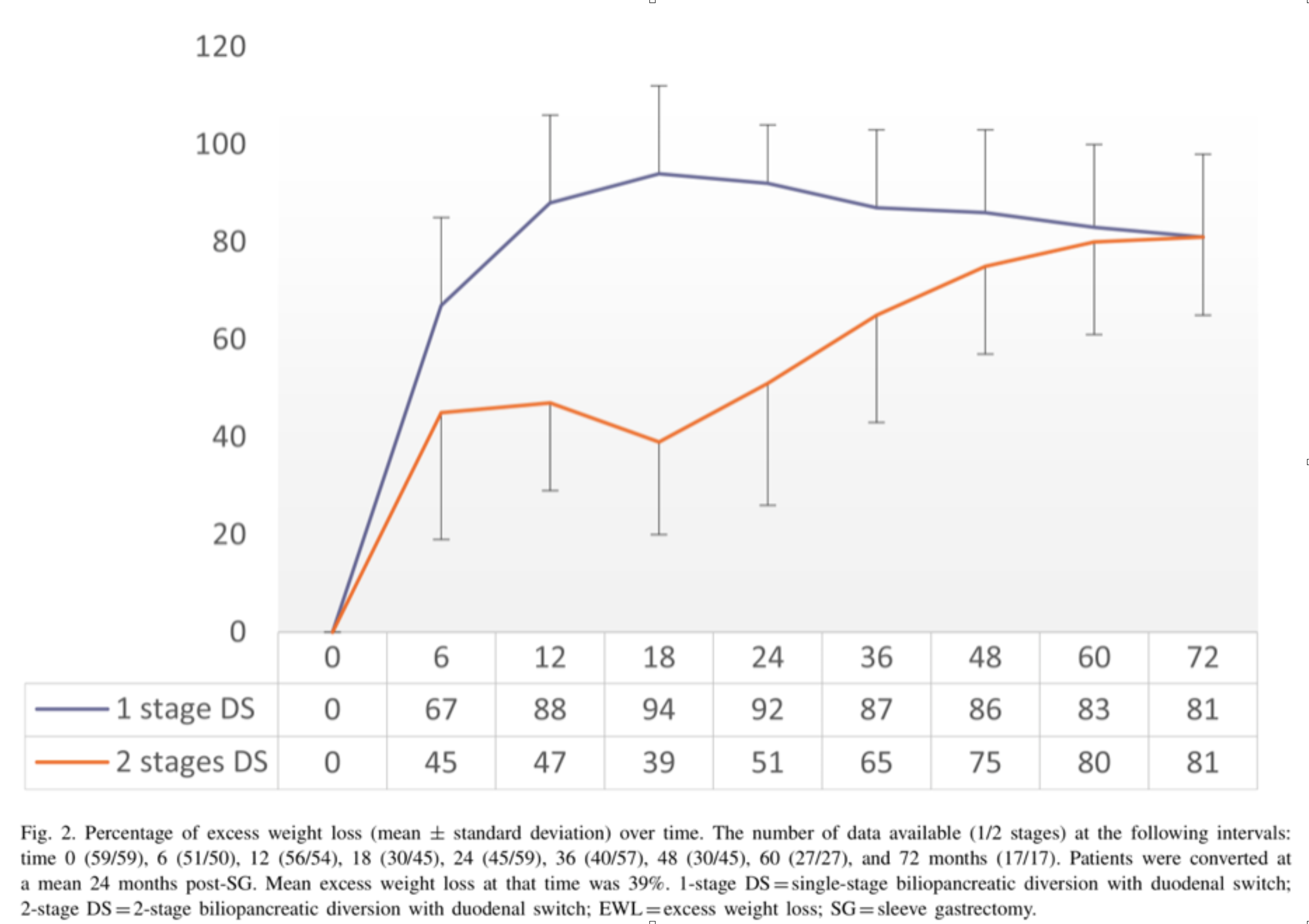
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
Health Insurances Working Against You
July 09, 2018 12:01 pm
Are Health Insurances working against you? Especially in people who have the disease of obesity? Insurance companies continue to lengthen the pre-operative period. The time that is required to lapse has now in some cases been extended between 6-12 months for some commercial health plans. There are yet again studies that have shown no benefit to the patient with this mandated waiting periods imposed on the patients. Unfortunately, the patients need to challenge the health care insurance companies by the means of all options that may be available to them. This may include internal appeal to external evaluation by some state agency. There are numerous studies that show pre-operative dieting does not equal better weight loss or compliance.


Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

New Pasadena Office Map and Parking
August 12, 2017 8:35 am
We’ve created a helpful map and parking diagram for our new Pasadena, CA office location. It also has a general layout of the Huntington Memorial Hospital Campus and Pre-operative intake and testing area. We hope that you find it helpful on your next visit to see Dr. Ara Keshishian, General and Bariatric Surgeon.

Dr. Ara Keshishian has performed more than 2,000 Duodenal Switch procedures, thousands of Sleeve Gastrectomies and more than 500 revisions from other Weight Loss Surgeries such as RNY Gastric Bypass, Adjustable Gastric Band, and Sleeve Gastrectomy to Duodenal Switch as well as General Surgical cases over the last 18 years of private practice.
Insurance Appeals And Denials
August 07, 2017 7:08 am
Whenever you are dealing with insurance issues it is important to have a general understanding of insurance ins and outs. The Obesity Action Coalition has a good general guide to the insurance process here. If you are having issues with out of network, out of area, or insurance appeals and denials for Duodenal Switch, there may be some additional assistance from two individuals who have had the Duodenal Switch procedure themselves. We are grateful that they have provided assistance throughout the years to the Duodenal Switch community. The following is their statement on insurance.
The majority of insurance companies are in the business of making money (for profit). They can deny requests for preauthorization with impunity. These denials are often complexly worded and difficult to comply with and overcome, and are definitely overwhelming to the patient, and the busy surgeon’s office. The vast majority of patients faced with demanding if not impossible to achieve prerequisites, or denial of the request for preauthorization simply give up, and the insurance companies pocket the savings.
If you find yourself facing impossible pre-op hurdles, or a denial, we urge you to appeal, and to seek assistance in preparing the appeal. You can hire an attorney, of course, but there is an informal and free resource we suggest that you investigate as well.
If you go to BariatricFacts.org (a non-profit, patient-run site), you will find individuals who are long-term DS postops, and patient advocates. They have been helping patients, pro bono (for free), for over 10 years. They will help you draft your appeal letters, provide supporting medical and legal documentation, and prepare draft letters of medical necessity to be reviewed and signed by your surgeon supporting your appeal. They will not represent you directly, but they will help you best represent yourself. in many cases it is necessary to exhaust all internal appeals (because the insurance companies are unlikely to overrule themselves), and then file for external review, where independent reviewers often overrule improper denials. If you join and then post on BariatricFacts.org asking for help, you will be connected with them and you can decide if you want their help.
Please note that this is just a suggestion. It is neither legal nor medical advice, nor a guaranty regarding their services, and you should always consider getting legal advice and assistance from an attorney who will represent you directly. The members at BariatricsFacts.org will help you draft your own letters, but will not be your legal or medical representatives; you will be required to do a fair amount of your own work on your appeals, and to sign them yourself.
It is suggested that before or at the same time as you contact the resources suggested at the site, you gather as much of the following information as you can:
- A copy of your Evidence of Coverage, which is the usually 100+ page insurance contract between your employer and the insurance company, which you can obtain it from your HR department. If you are self-insured, it will be available directly from your insurance company. Note: it is NOT the Summary of Benefits – it needs to be the contract itself.
- If your insurance is through an employer, you need to determine whether your plan is self-funded or fully-funded. Your rights are significantly different under the two types of plans.
- If your insurance company has a separate bariatric surgery policy, provide a copy of that, too.
- A copy of your surgeon’s request for preauthorization, which provides the ICD-10 and CPT codes submitted.
- A copy of your denial letter, including the section regarding your appeal rights.
* It is strongly recommended that you obtain a copy of your surgeon’s LOMN (letter of medical necessity) before it is submitted to your insurer or for external review, so we can assist your busy surgeon in making the strongest possible case for you.
Don’t be deterred by a denial. It is unfortunately more common than it should be, but it can often be overcome if you meet the requirements for bariatric surgery, if you get help navigating the process.
Shared Success Story- Theresa & Rodney (Duodenal Switch)
August 05, 2017 8:41 am
Life before surgery seems like a lifetime ago for both my wife and I. Being extremely overweight is not only a burden on your general health but a burden on your lifestyle in general. You have the awful label of being called obese, or morbidly obese. This is such a wonderful word that makes you feel as if you have been judged a misfit in society. We were both overweight all of our lives and had done all of the diets known on the planet throughout the years. Some worked a little some not at all and we always found ourselves back to where we were before and usually larger than that. The main focus though as we were getting older was our health. For Theresa it was very difficult. Along with being over 400 pounds she had a severe case of asthma which caused her episodes where she felt she was going to suffocate. She also had very little muscle mass which made it very difficult to get up and down from seating or lying positions. Theresa had her surgery in February of 2014 and not a moment too soon. If she had done nothing it is a good chance that she was facing a horribly short future. She also has a slight heart murmur which did not bode well for a person with her weight. She did not have diabetes thank goodness but her A1C was on the rise as was her BP. She did have sleep apnea as well and had to have a CPAP machine.
I was also severely overweight, my highest weight was nearly 400 pounds and on surgery day I was 355 pounds. I was also under the illusion that I had more control over my weight and that once Theresa had her surgery I would just be able to diet and exercise my way to a healthy weight. I was able to do this in my younger years to a certain extent and I was naive enough to think I could continue to do so. How wrong I was. I had found that no matter how much diet and exercise I did my weight would drop a bit at first but then stall and I would have to essentially starve to lose any more and of course that just makes for a bad outcome. My A1C shot up to 7.6 and this was with 1000mg of metformin a day! My BP was very high with both numbers over 100, well over. This is with a high dose of BP meds. I had a severe case of sleep apnea and could not even consider sleeping without a CPAP machine with a high pressure. I have an artificial hip that was being burdened by my 350 pound plus frame and would probably need to be replaced sooner rather than later. My future was not looking good. Dying before I was 60 seemed like a reality for me and that is not the future I was hoping for. The decision to have weight loss surgery for the both of us was tough. You of course hear the nay sayers spout what a cop out it is and it’s the easy way out! You are just weak and just simply need to not eat hamburgers, French fries and donuts. Just stick with non-fat and low calories and you will reach the promised land. What a load of BS.


Once you wrap your head around the fact that your body is wired in such a way that it will always seek a higher weight every time you lose weight, it’s time to consider the type of surgery. Everyone has heard of the Gastric bypass and that seemed to be the path at the time of Theresa’s surgery. The thing about Theresa and what I admire very much is her persistence and her ability to research to the point where a decision is spot on. She looked at all of the four possible surgeries and quickly realized that the Duodenal Switch was a no brainer. It had the greatest measure of success in the long term as well as short term. Reading about the process and talking to others who have had the surgery it became clear that it was the right choice. Finding out where to go and have the surgery was a real challenge. We were lucky to find Dr. Ara Keshishian and have the ability to travel to his location to have the surgery.
Theresa’s Stats Rodney’s Stats
Surgery Weight: 410 Surgery Weight: 355 Pounds
Total Weight Loss: 215 pounds Total Weight Loss: 170 Pounds
Surgery Type: Duodenal Switch Surgery Type: Duodenal Switch
Surgery Date: February 2014 Surgery Data: May 2016
Surgeon: Dr. Ara Keshishian Surgeon: Dr. Ara Keshishian
Life after surgery is an amazing series of challenges, changes, and a journey that transforms your life in a huge way. For Theresa, it was freedom. Freedom from the overbearing weight she was carrying that kept her from essentially moving or doing anything but staying at home. We did very little outside of the house before surgery. Only the necessities of shopping and keeping up the house on the inside and out. Even that was difficult and went by the wayside all too often. Of course eating out was easier than going to the grocery store and that made the scale just go higher. After surgery, Theresa began to lose weight and you could see day by day the changes. After the first month, you could see a dramatic change not only in her look but the fact that she was moving again! She had dropped 35 pounds in that first month and it made a huge difference. As the weight kept coming off over the next few months we began doing things we have not done before. We started to do a lot of walking and a lot more things around the house that needed to be done. Shopping became a breeze and we ate out a lot less. The dramatic change was in her health. A number of changes for the better were happening on that front. The main one and a huge relief was the asthma. It simply was no longer there. She was no longer short on breath and was simply out moving me! I could barely keep up with her. She also had a bad case of psoriasis which before surgery she could do nothing about. Since the surgery it has disappeared. It might be due to the increased in vitamins, particularly the D vitamin. Her sleep apnea went away and now she is healthy and happy. It is almost difficult to describe the changes until you see them for yourself. For Theresa it has been a life changing experience that has transformed the both of us in ways we never imagined. Theresa eats a normal diet and after 3 ½ years post op she fluctuates about 5 pounds either way. It is amazing.
For me it was not what I expected. What I mean by that is, learning to eat is a challenge. With the Duodenal Switch you are not only eating less, but what you eat is tremendously important to the success of the transformation. With the other surgeries, Lap Band, Bypass and Sleeve you do not have the degree of malabsorption. You simply eat less and you lose weight, but you are still essentially “on a diet”. With the Duodenal Switch you have to consider the malabsorption and think protein first and for most. Once you get past the first month of eating small amounts and what you can while your innards heal you need to learn what to eat and is it enough protein. You may also have to contending with the fact that you have an aversion to foods you ate before. I, for one, could not even eat cheese, and chicken. I pretty much lived on scallops, crab, shrimp and protein drinks for the first three months. Nuts were also a good source of the protein when you get to that stage. This does change and things do go back to normal as far as the taste changes, but it takes a few months. The weight in that first month pretty much peeled off. I was dropping like a pound a day. It was incredible. You think that this is going to be a breeze and you will drop it all in no time! Then that 4 week somewhat of a stall occurs. From what I can tell, everyone experiences it in one form or another. It freaks you out because you start to think about the past where you would work your butt off and either gain or drop and ounce or two. But I was lucky, my wife had gone though it two years before me so she was there to explain that it was normal. The whole “this is a journey thing”, and she was right! At the time though I was listening to the negative voice in my head from the past. That is where the support from the many groups come in. You see that pretty much everyone has the same ups and downs and then your body gives up the farm and you drop a bunch of weight in a weeks’ time. There is really a lot of science behind it. Researching and reading about this particular surgery and how it works will benefit you while you go through the process. Another important thing we face with this surgery is the necessity of Vitamins. Thank goodness for my wife and the DS groups and of course my surgeon. You will not be without knowledge if you actively join the different groups and do your research on the vitamins. I am still learning about what my body needs and am looking forward to my labs in the next month to see where I may be deficient. I have also come to realize the importance of drinking water and avoiding dehydration. I never used to drink it much before the Duodenal Switch, but since the surgery I find it aids heavily in the success if you drink it and drink a lot of it.
To conclude this has been a journey and one I wish I could have done a lot sooner in life, but it is never too late. Today Theresa and I are at weights that we are happy with and our bodies are happy with. We are more active then we have ever been before together. No more days idle in front of the television with large amounts of fast food and drinks. That is what we used to look forward too. Now we cannot wait until we go out and do something. We are not running marathons or anything but we are active and enjoy being so. We no longer have the ailments we had before surgery. Theresa’s asthma is practically nonexistent, living in the northwest with fires in the summer she may have a bout or two. Nothing even close to what she has before and a simple inhale and its gone. Both of us no longer need a CPAP! The freedom to simply lay your head on the pillow and sleep is amazing and wonderful. All of the medication we had prescribed for us are gone as well. My A1C was 5 on my last set of labs and 5.3 on the one before that. Theresa’s is the same and has been for three years. BP is normal and my hip is holding steady. Oh, and another cool thing about it is you can actually shop for clothes anywhere! Your sizes will shrink but we have found we have become quite the clothes horses since losing all this weight. It makes it fun to be able to fit into a size you haven’t seen since who knows when.
Life is always a challenge for many reasons but to remove the burden of the weight simplifies things just a bit. It is a decision we will never regret and wished we had made a long time ago. We both owe our lives firstly, to having Duodenal Switch surgery. Secondly, and most important – was in seeking out the best surgeon we could find, and that was without a doubt, Dr. Ara Keshishian. As a surgeon he is thorough, meticulous, constantly learning and keeping up on the latest research;as a person he is easy to talk to, very approachable, and genuinely cares about his patients before, during and after the surgery process. We could not imagine choosing anyone else.