Category: Gastroparesis
Bile Reflux Gastritis
May 19, 2026 4:13 pm
Hello, it’s best to clarify a few points:
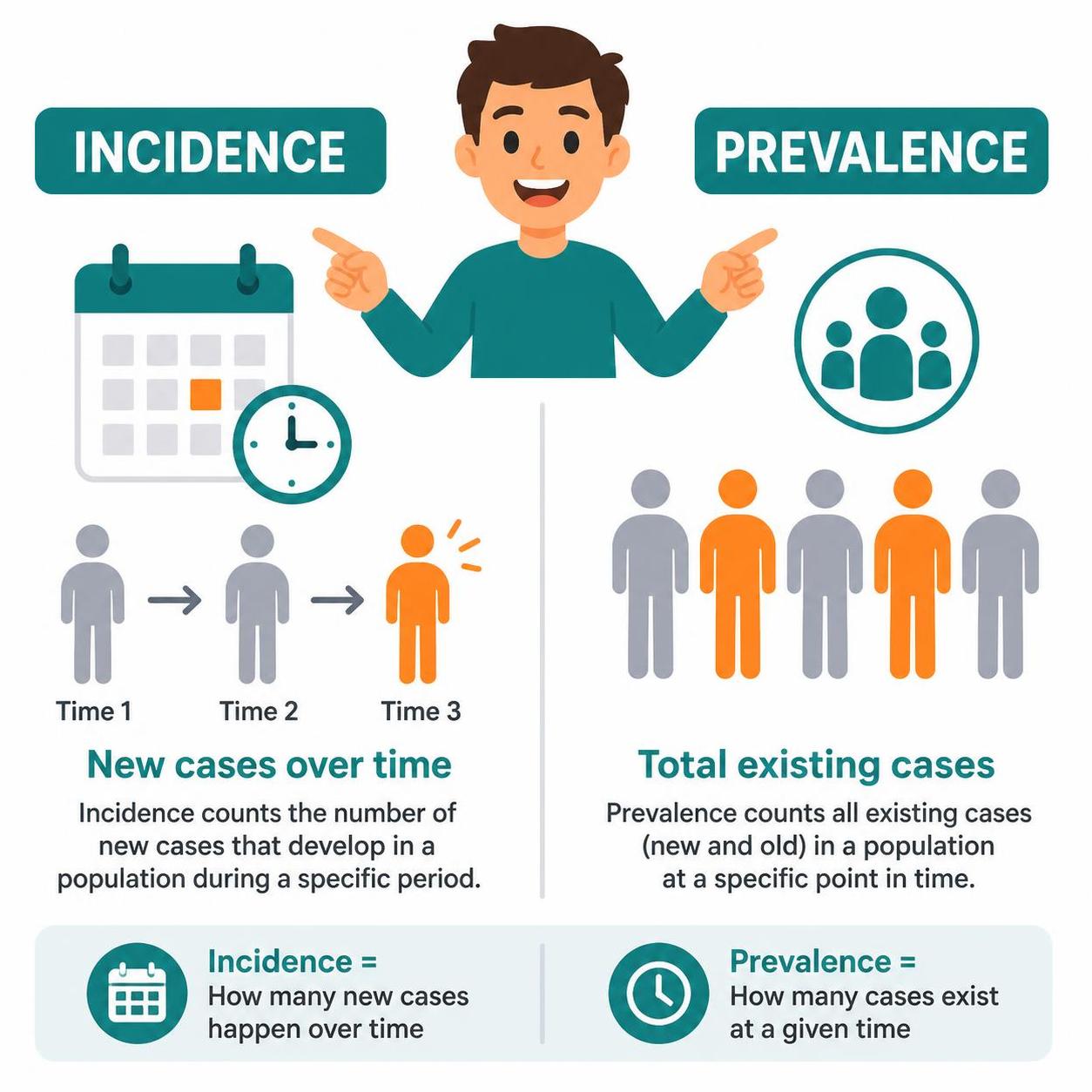
- The difference between prevalence and incidence.
- Incidence means new cases over
- Prevalence refers to existing cases at any time
- The difference between causation, coexistence, and correlation
- Causation refers to a condition causing an effect.
- Coincidence refers to two conditions present together at the same time, with neither causing the other.
- Correlation refers to two conditions that may occur together, with no causation.
- Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
- Confounding factors.
Three Different Problems: Gastritis, Gastroesophageal Reflux, and Bile reflux Gastritis
June 05, 2025 4:52 am
Gastritis is a general term used for the description of symptoms associated with several very different physical conditions and require different treatments based on their ideology . Gastritis, gastroesophageal reflux, and bile reflux gastritis
Gastritis may be caused by excess acid or bile in the stomach. Some patients may have gastroesophageal reflux due to a hiatal hernia, which needs to be treated surgically with Nissen fundoplication, regardless of the size of the hernia, contrary to what gastroenterologists recommend by prescribing antacids for an extended period. I have seen patients who have had one cm hiatal hernia and have been very symptomatic, and others who have had larger hiatal hernias and have been asymptomatic. Size should not be a determinant of whether the patient has had or will have a hernia repair or not.
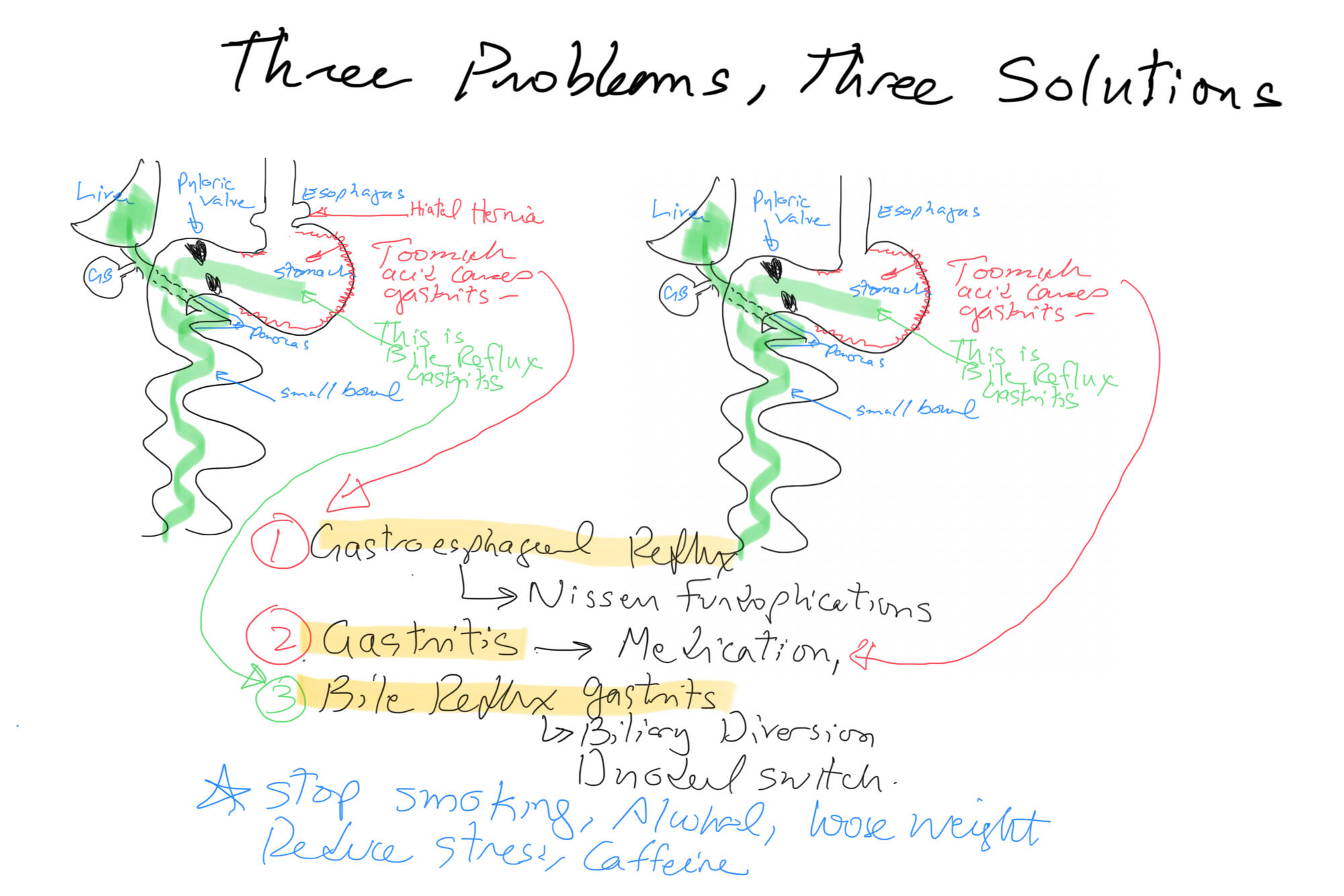
Billiary Diversion is the definitive surgical procedure for Bile Reflux Gastritis.
Bile Reflux Gastritis and Cholecystectomy
May 21, 2025 2:41 pm
Bile reflux gastritis is not a the result of the cholecystectomy but may be seen in a subset of patient with other confounding conditions. Bile is produced in the liver and stored in the gallbladder. In response to high fat and protein in the stomach, the gallbladder contracts to ” squeeze” the bile stored in the gallbladder into the small bowel to help absorb the fat and protein.

With the gallbladder removed, the bile produced by the liver cannot be stored and goes directly to the small bowel via the biliary tree.

It is possible and likely that some of the bile will find its way back to the stomach. In some patients, due to compounding circumstances, the bile may collect and cause gastritis. We need to dissect this a little for it to make sense.
- Not every patient after cholecystectomy will have bile in their stomach.
- Not every patient with bile in the stomach has gastritis.
To appreciate this, let’s remember that for bile to get from the small bowel to the stomach, it needs to:
- Go upstream, against the peristalsis of the small bowel, and do not be washed down by the flow of the gastric
- juices coming out of the stomach.
- Go through the pyloric valve.
- If it reaches the stomach, the acid in the stomach does not neutralize it, causing gastritis.

As I’m sure we all appreciate, other contributing factors besides cholecystectomy may cause bile reflux and bile reflux gastritis. This is why it’s also emphasized that bile in the stomach alone does not confirm biliary reflux gastritis. It is also why we always state that bile reflux gastritis is a disease of exclusion, where other conditions such as gastroparesis, acid reflux, and hiatal hernia (regardless of size, as some patients are unfortunately told that since the hernia is small it does not need to be fixed, which is incorrect) must be considered. Further information on Bile Reflux.
Billary Diversion is the only definitive surgical procedure for Bile Reflux Gastritis.
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
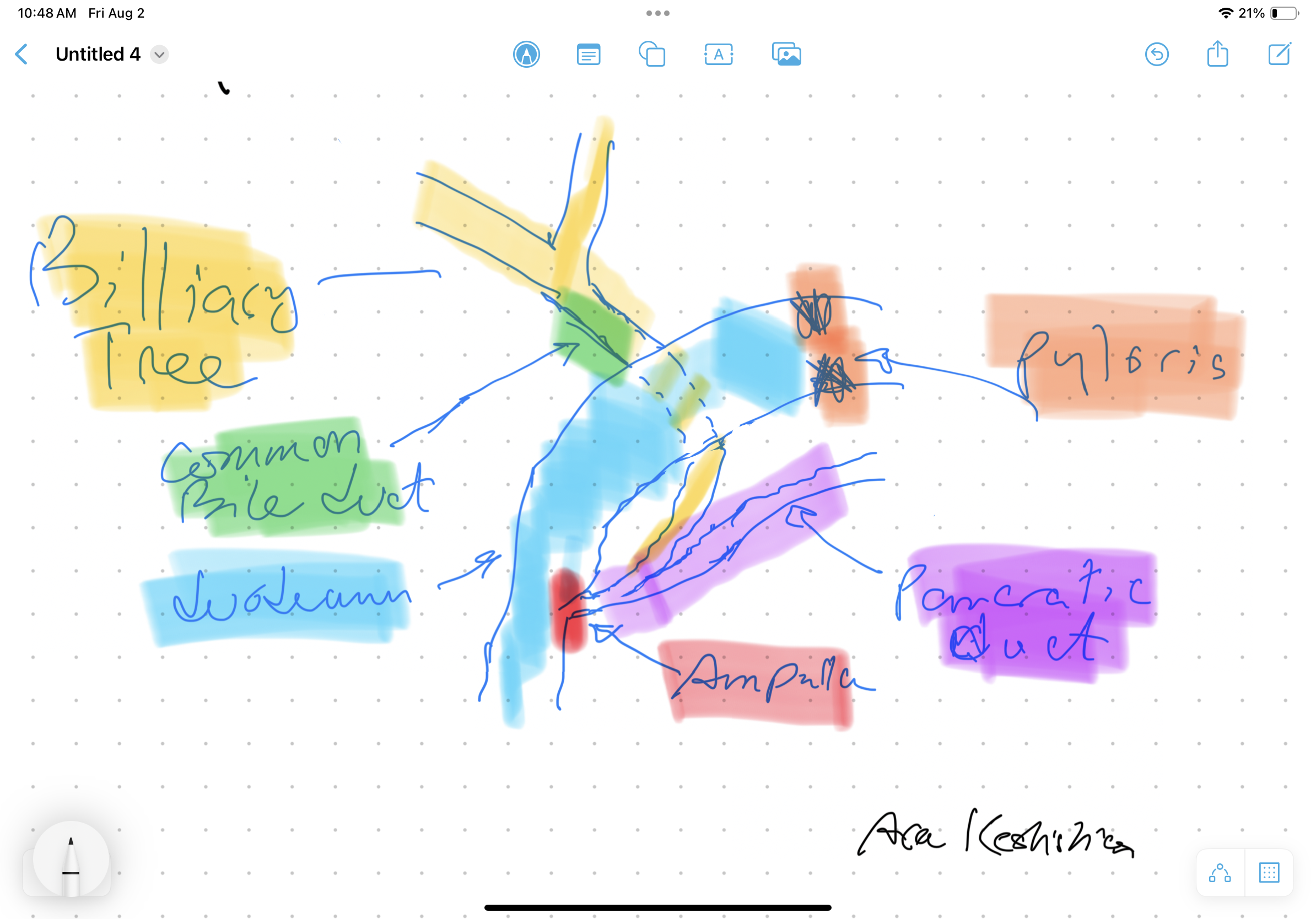
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

Bile Reflux Gastritis
January 10, 2018 1:45 pm
Bile reflux gastritis has been recognized as a significant cause of dyspepsia in a subset of patients. This patient group set does not respond to the standard treatment (not expected to) and some get improvement with the treatment of H.Pylori infection if one is diagnosed at the time of upper endoscopy and biopsy.
Inflammation and Foveolar hyperplasia are some of the findings that can be seen endoscopically. This and other findings have all been documented in the literature. An article published in 2005, reported over 40% incidence of Foveolar hyperplasia in patient with bile relax.
It is been noted that bile causes the thickening of the mucosa lining of the GI track. This is called Foveolar hyperplasia when the mucosa of the stomach is noted to be thicker with more numerous and deeper folds.

The treatment for this is reduction and prevention of bile reflux to the stomach, in some cases this can only achieved by surgical diversion of the bile from the stomach. Additional information on Bile Reflux and the surgical treatment can be found here.
Dual Testimonial: Cameron’s Gastroparesis surgery & Scott’s Revision of a Duodenal Switch
February 01, 2016 8:04 am
In 2015, I came into contact with the most unique, passionate, urgently responsive; talented beyond belief and caring surgeon I have ever met. Our oldest son who is a 21-year-old cancer survivor, has had nearly five years of medical nightmare as diagnosed with severe gastroparesis resultant from his vagal nerve being severed during a previous Nissen Fundoplication surgery. We didn’t find out that this had happened until nearly two years later and only after a 4 hour gastric emptying test showed that Cameron’s stomach was only about 30% emptied after four hours (should be empty after an hour) due to gastroparesis.
I had heard about Dr. Keshishian on a Bariatric support group page on which I post and get great advice. The surgeon back in Central, IL where we live told us that Cameron needed a subtotal gastrectomy to remove 80% of his stomach! This sounded radical and no way in the world was that going to happen. I was given Dr. Keshishian’s email address so I could consult with him for his advice. It was a Saturday morning around 7 AM Central time when I sent off an email to Dr. Keshishian detailing Cameron’s medical history and current issues. I was in hoping that his office would get the email on Monday and hopefully get back to me within a week. I went out to my kitchen to get a cup of coffee and when I returned I had a missed call with a California area code. Yep, it was Dr. Keshishian. I called back and we talked for 45 minutes. He suggested several things and told me that any good general surgeon in my area could do surgery on Cameron and fix him, well that was the only time he was wrong. We couldn’t find anyone in our area who would do the surgery.
So we talked and agreed that Cameron needed a Roux-en Y drain put in place to physically drain his stomach by way of gravity (not for any weight loss as very little small bowel was bypassed). Dr. Keshishian got us in the next week and we flew out to Glendale where he met with Cameron for an examination on that Monday. On Tuesday, Dr. Keshishian performed surgery to fix Cameron’s herniated diaphragm, loose Nissen wrap, performed the Roux-n Y limb and anastomosis to the stomach. Dr. Keshishian also found a Meckel’s diverticulum (a congenital small bowel defect that can cause internal bleeding and serious issues). The following Sunday, Cameron developed severe pain due to chronic pain from his Cancer treatment and 12 subsequent surgeries, many on his abdomen. Dr. Keshishian saw Cameron in the ER and spent 3 hours fixing Cameron’s pain issue and making sure he was medically sound so we could fly home the next day.
Today, Cameron has very little to no issues which you wouldn’t have believed possible six months earlier. In the past, he had violent retching, dry heaving and bad nausea daily which had him severely incapacitated and very depressed due to a feeling of hopelessness and pain from the Gastroparesis. He didn’t believe he had a chance at a normal life but Dr. Keshishian gave Cameron his life back. We are eternally grateful for your huge heart and talent Dr. Keshishian. Thank you!
During our time in Glendale in 2015 for Cameron’s surgery Dr. Keshishian and I began discussing my situation. I had been given a virgin Duodenal Switch performed by a surgeon in Illinois in September of 2013. A year later in 2014 and 180 lbs lighter, I ended up in the hospital as I was passing out. I had a resting heart rate of 35 BPM, a blood pressure in the 75/40 range and incredibly bad labs including anemia, low copper, low zinc, and dangerously low albumin and total protein. A full cardiac work up was completed and I spent a week in intermediate care. Why? I was extremely malnourished even though I was consuming 200-250 grams of protein daily! Why was I malnourished? Because my original surgeon performed a “cookie cutter DS” on me where he didn’t measure my small bowel and arbitrarily gave this 6’2 man a 100 cm common channel and a 150 cm Alimentary limb. Way too short on the AL! Had the Hess method been followed (the only way the DS should be allowed to be completed) my CC would have been 100 cm (that was okay) but my Alimentary channel should have been 275 cm! Simply put, my absorbing portion of small bowel was 34% and the Biliopancreatic limb (non-absorbing) was 66%. It should have been a 50/50 ratio with 100 cm CC, 275 cm AL and a 375 cm BPL. In order to combat my severe malnutrition that September of 2014 I went on a pancreatic enzyme (CREON) to assist my nutrient absorption. I was taking with meals right around 400,000 IU’s of CREON (a boat load) and this was barely keeping my nutrients in range and lab values barely in range. After speaking with Dr. Keshishian, he recommended that I give it until around September of 2015 to see if my absorption increased enough to where a revision wouldn’t be required. Towards the end of July, I all of the sudden lost nearly 20 pounds in two weeks from my already frail and scrawny body. I saw my surgeon in Peoria as I was very alarmed; and I had been having bad cramping and other issues point to a possible bowel obstruction His exact words to me were “see me in 30 days, you are like the DS poster boy of good nutrition”. As you can imagine I found that completely unacceptable and soon as I was out of that appointment I emailed Dr. Keshishian. He told me that if I couldn’t get a revision ASAP I would need to immediately go on TPN. Two weeks later my wife and I landed at LAX and were in Glendale on Monday morning for an exam with Dr. Keshishian.
The job Dr. Keshishian did describing what he was going to do, and of course this was a visual presentation with Dr. Keshishian drawing (you know Dr K’s love of drawing) out for us what he was going to do. He thoroughly explained for my wife and I so she was comfortable with what was going to happen and we fully understood what he was going to do. Doc also found an umbilical hernia that he was going to repair and I had an anal fissure as well that wouldn’t heal so we discussed what he would do to examine and possibly fix during my revision surgery. The next day Dr. Keshishian performed surgery where he fixed the umbilical hernia, measured my total small bowel length to determine appropriate channel lengths and found an repaired a huge mesenteric defect (intestinal hernia and Dr K has a picture of my guts with the huge hole in the mesentery that he has posted on his blog discussing intestinal hernias and blockages), fixed my fissure (Thank you!) and put in a side by side anastomosis that effectively lengthened my AL by 125 cm and my CC by 25 cm worth of absorption. This put my absorbing intestine to BPL ratio where it should have been in the first place (50/50 ratio).
I am pleased to say that I immediately went off the CREON and my absorption and subsequently my lab values improved tremendously. At surgery on August 18, 2015 I weighed a whopping 170 lbs. Today I am weighing in at 183 pounds and well on my way to Dr. Keshishian’s suggested optimal weight target of 205.
Dr. Keshishian is absolutely amazing and the best in the world when it comes to performing the Duodenal Switch and revision to DS Surgery (Band to DS, RnY to DS, Channel extending revision to DS). I would recommend Dr. Keshishian to any patient who needs a virgin Duodenal Switch to get their health back and especially to those who were sold a garbage RnY or Crapband procedure that ultimately failed you (it failed you, you did not fail). In fact, I am trying very hard to convince my brother and Step Mother to fly to Glendale and have Dr. Keshishian perform a Duodenal Switch on them. They very much need it for their health and Dr. Keshishian is the best in the world having performed over 2,000 DS procedures.
I don’t say this lightly. Ara, you are one of the finest human beings I have ever had the good fortune of knowing and your surgical skills are second to none. I really do admire and love this gentleman like a brother and consider him to be a friend. Thank you for using your incredible skill to fix my health issues resultant from the failed cookie cutter Duodenal Switch I was given two years earlier by another surgeon. Had I met you back then and knew what I know now, you would have performed my virgin DS and I would not have suffered for two plus years. Thank you from the bottom of my heart, Dr. K!