Covid-19 Pandemic and Obesity
April 12, 2020 7:44 pm
We have now seen several articles with data collection regarding patients with obesity and COVID-19 being at greater risk of hospitalization. We can look at metabolic syndrome associated with obesity as a risk factor also.
We have all been in physical isolation due to Covid-19 pandemic. The strategy of minimizing contact has worked. The data is clear when comparing information from states that instituted an aggressive containment plans compared to those who have not. This shows a sigifnicat flattening of the curve in California for example.
The CDC publishes the Morbidity and Mortality Weekle Report (MMWR) . The latest publushed summary (as of date of publucation of this blog) provides an insight to the risk factors of hospitalization.
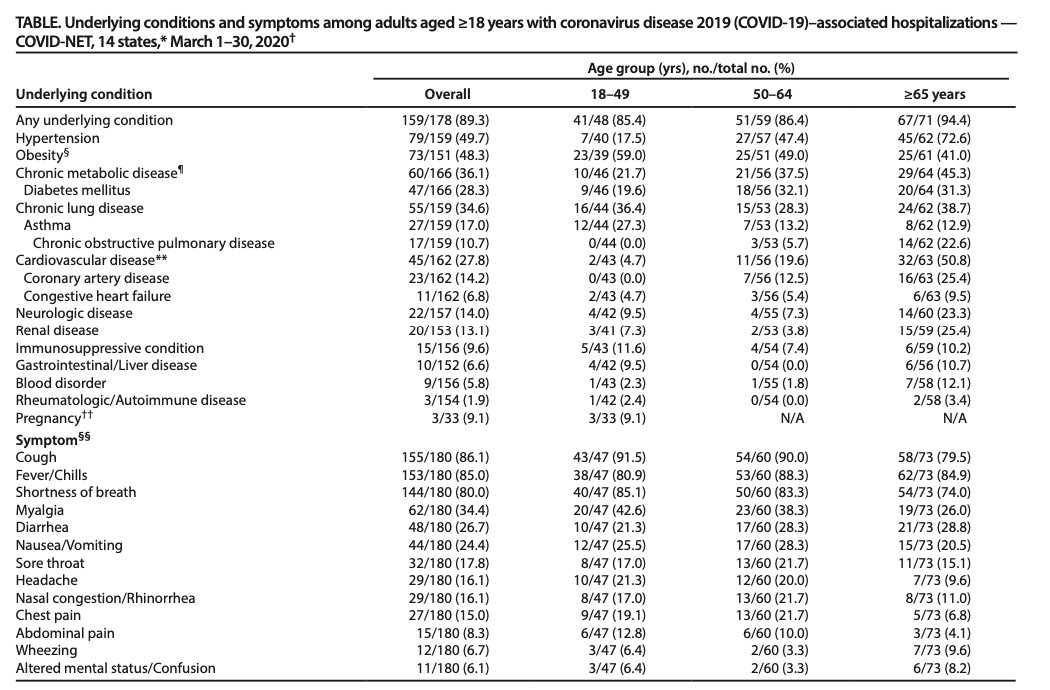
Concerning to see that a respiratory virus is more likely to hospitalize those with Obesity, Diabetes and hypertension at a higher rate than lung and pulmonary related conditions.
Let us recognize that this is only a summary collected data. Therefore, there are limitatation to making any assumption of conclusion based on this information.
With those limitation aknowldged, and relying on our obesity related comobidities, we can make a few conclusions:
Not surprising, Obesity as with other diseases, compounds Covid-19 exposure and infection. Diabates is also a risk factor. There are no indepth information available on the diabetic patients. There is now data showing superior outcome of diabetes resoultion with weight loss surgery compared ro medical treatment.
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
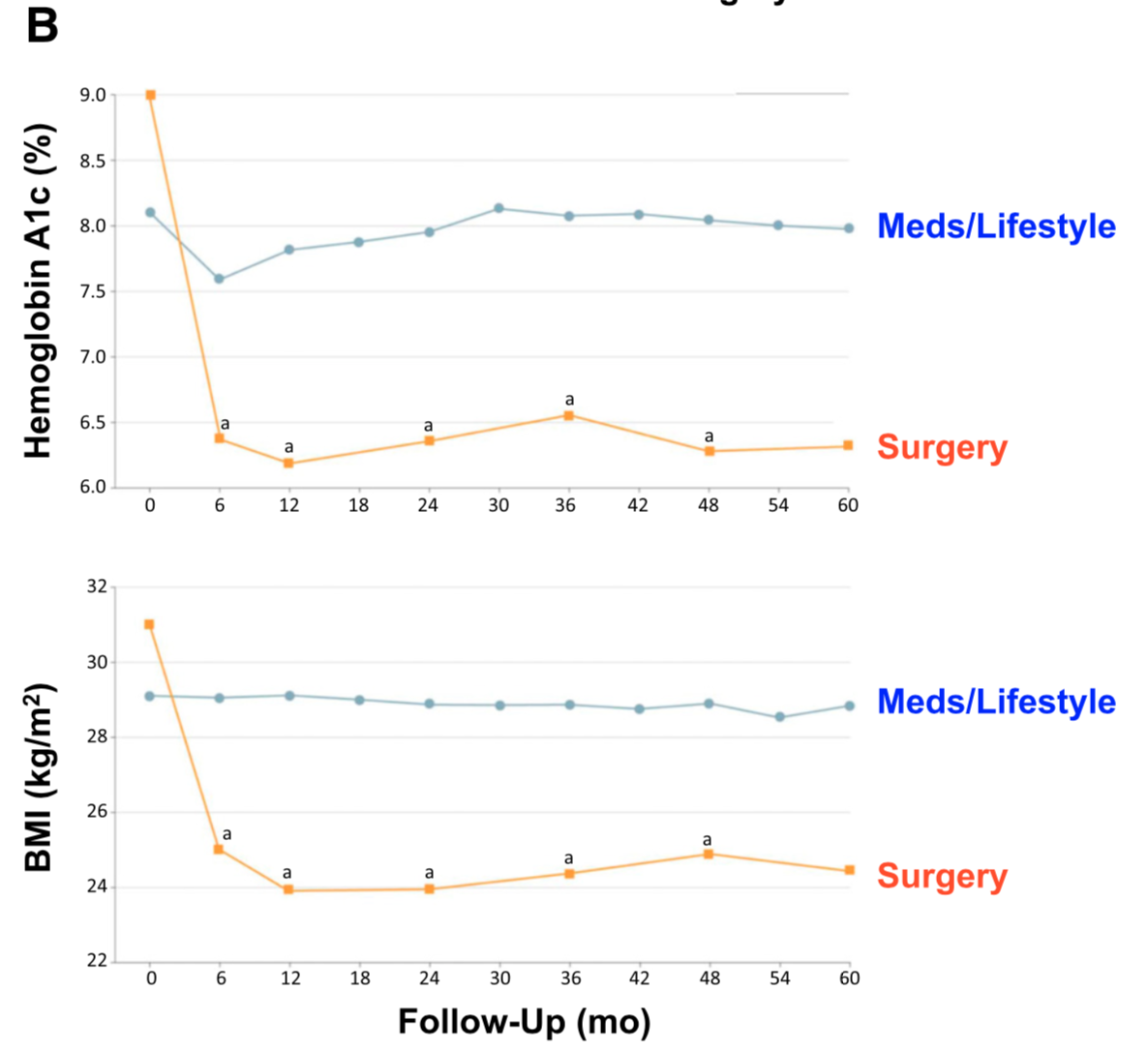
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.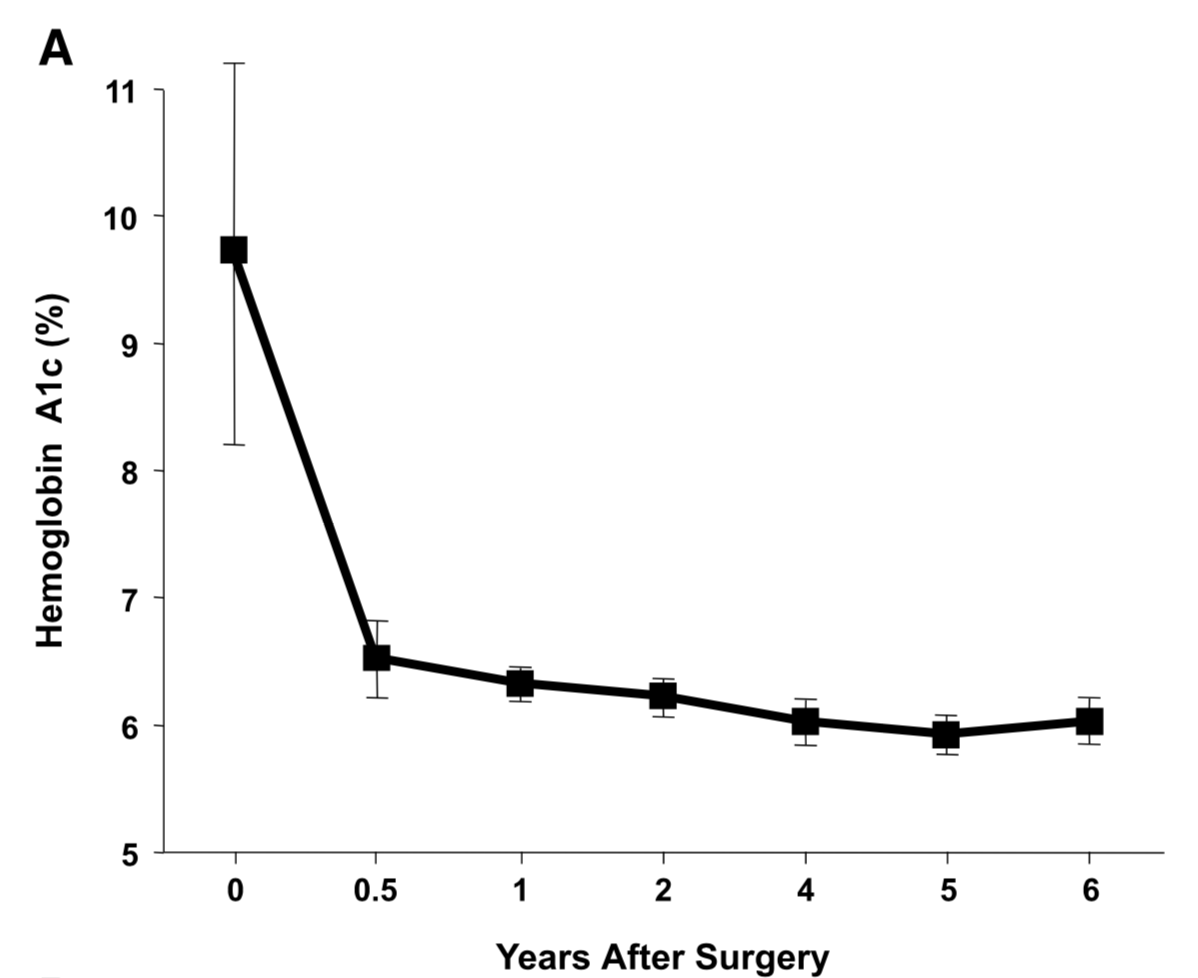
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
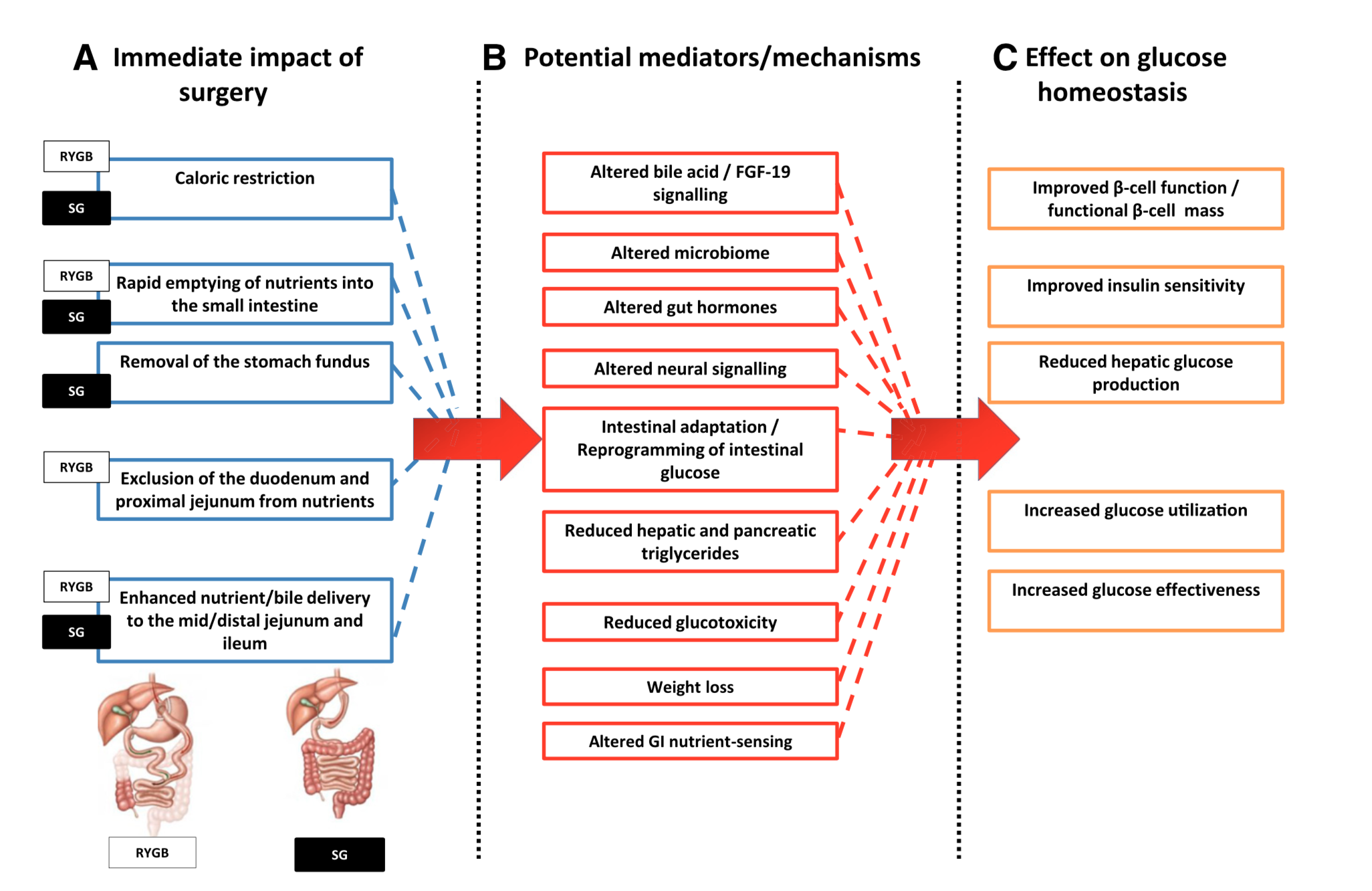
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Medication Absorption After Weight Loss Surgery
March 30, 2020 8:01 am
Weight loss surgical procedures, in one form or another, achieve the desired effect of weight loss by altering absorption of fat, protein, and carbohydrates. This results in decreased total absorption of required calories.
An unintended consequence is the altered absorption of medications. Frequently I am asked about the specific medication. Usually the answer is vague since the information is limited on specific medications. If the desired effect is not achieved, then it is probably not being absorbed well. Specially, if the same dose of the same medication working well before surgery.
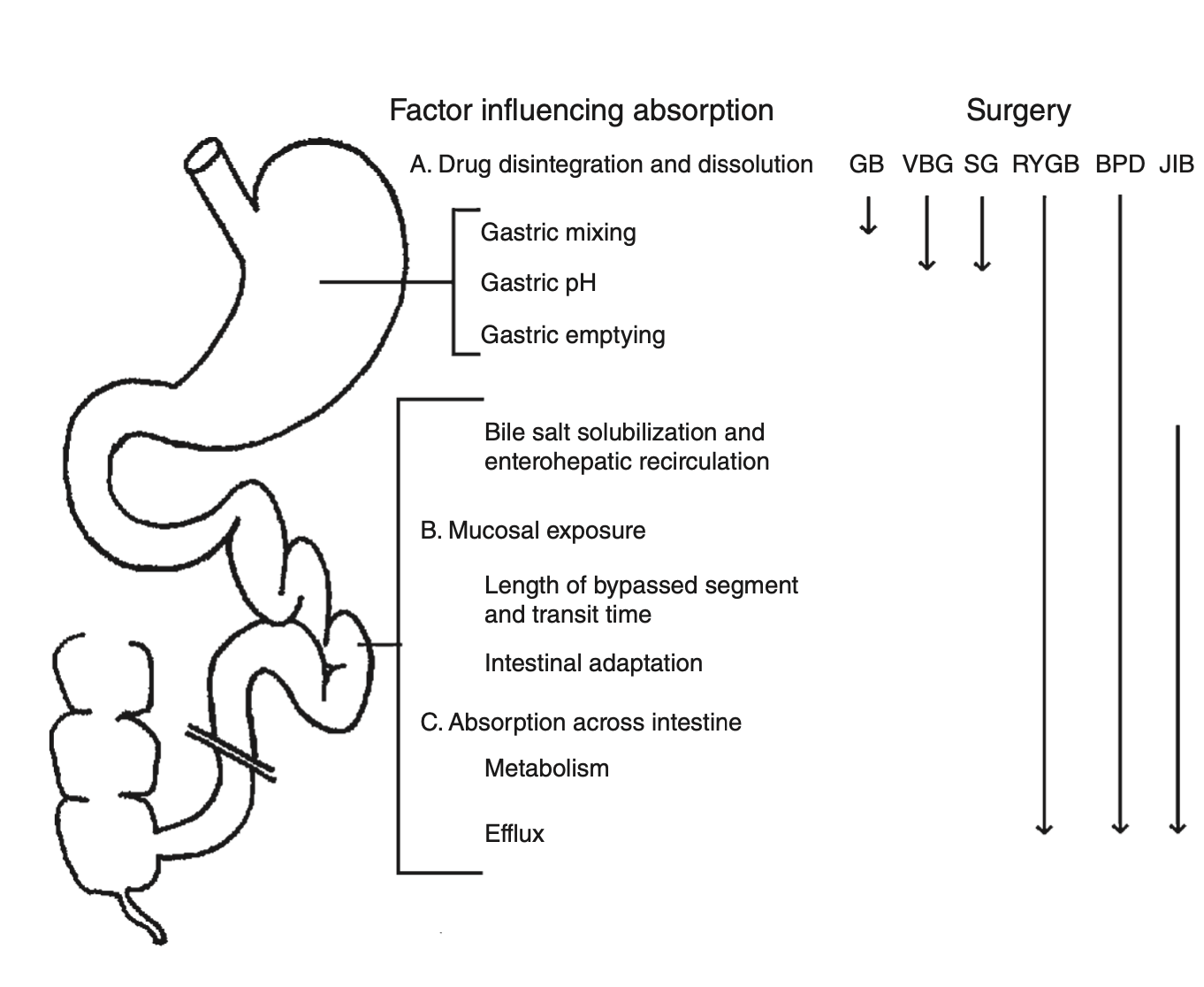
There is a summary article about the Theoretical absorption pattern of different weight loss surgical procedures.
Osteoporosis Medications
March 28, 2020 7:22 pm
There are a number of lectures, posting that we have done over the years on this topic. However the questions of osteoporosis medications and their benefits and risks comes up often.
The links are attached:
Here is an updated list of medication that I had previously published. I made some clarification to explain how the medications work. There are different classes of medications and the detail of the action and soda effects were described earlier at a blog post.
List of medications that effect bone health.
The table is obtained from https://www.nof.org site.
Pregnancy File
March 28, 2020 9:08 am
Other Pregnancy Info:
Research regarding pregnancy after WLS:
PCOS, Fertility and WLS:
Vitamin D Metabolism and Deficiency file
March 28, 2020 8:17 am
It’s important to understand Vitamin D metabolism and deficiency potential following weight loss surgery Vitamins after DS need to be followed via laboratory blood studies. There are basic vitamin needs but individual needs should be based on medical history, genetics, alimentary limb length, common channel length and other surgical and physiologic determinations. Vitamins after DS are a life long commitment as well as protein needs and hydration. Duodenal Switch is a malabsorptive procedure which requires at least yearly laboratory blood studies, daily vitamins/minerals, daily high protein and daily hydration intake. There is not an all in one vitamin that is adequate for a DS patient or tailored to your individual needs. (example: you may need more Vitamin D and less Vitamin A if you are taking a all-in-one vitamin you can’t get more of one and less of another vitamin)
DS patients are recommended to take Dry forms (water miscible form) of Vitamin A, D3, E, K due to the fat malabsorption after DS. Dry formulations by Biotech are processed so they can be absorbed by a water soluble method after the DS procedure. Vitamin D seems to be the vitamin that can become deficient the easiest, followed by Vitamin A. Take these vitamins away from dietary fat.
In some cases, patients may need injectable Vitamin A or D to improve vitamin levels.
Click the links to view the information below and within the comments of this file:
Vitamin D3 50 by Biotech: Amazon
directly from BioTech:
Many DS surgeon’s do not recommend Children’s vitamins or chewable vitamins unless there is a specific reason or need for them.
DS Surgeon Blog on Vitamin D:
Webinar on Vitamin D metabolism:
Medications that effect Bone health:
This does not constitute medical advice, diagnosis or prescribing. It is simply a compiled list of gathered information. If you are in doubt or have questions please contact your medical healthcare professional.
Articles
March 22, 2020 6:57 pm
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
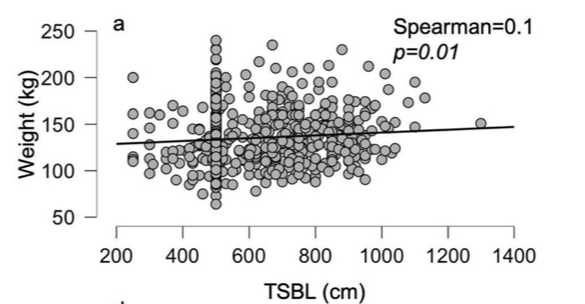
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
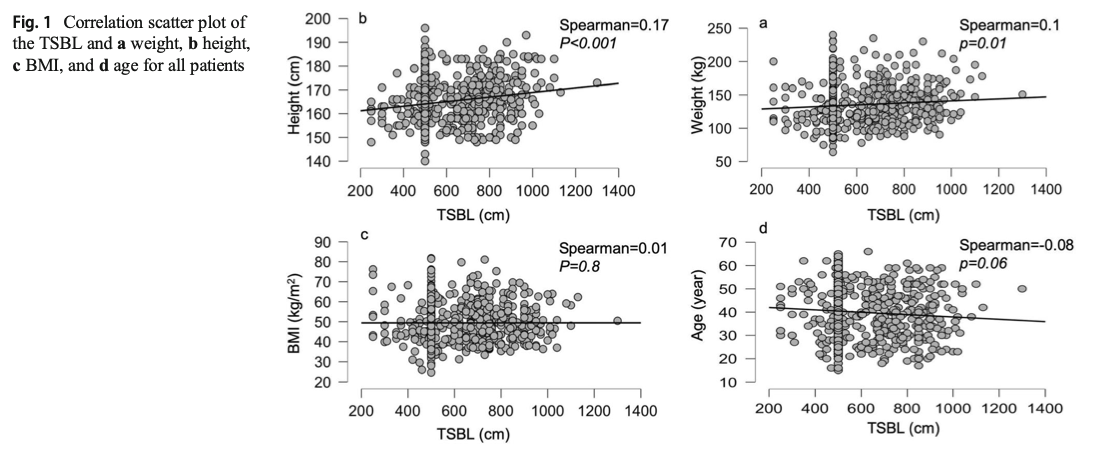
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
Stop The Spread of COVID-19
March 22, 2020 3:18 pm
Symptoms of Coronavirus Disease 2019
March 22, 2020 3:09 pm
Some of the common symptoms of Coronavirus disease 2019 infection may range from mild “Flu” symptoms to shortness of breath and high fever. Please check CDC.gov for frequently updated information.