Added Sugars: Now Listed on the Nutrition Facts Label
December 07, 2020 9:46 pm
In March 2020, the Federal Food and Drug Administration updated the food labeling requirements. Therefore clarifying the information. This was to simplify and improve the information provided to the consumer.

COVID – 19 Vaccine explained
December 07, 2020 9:10 pm
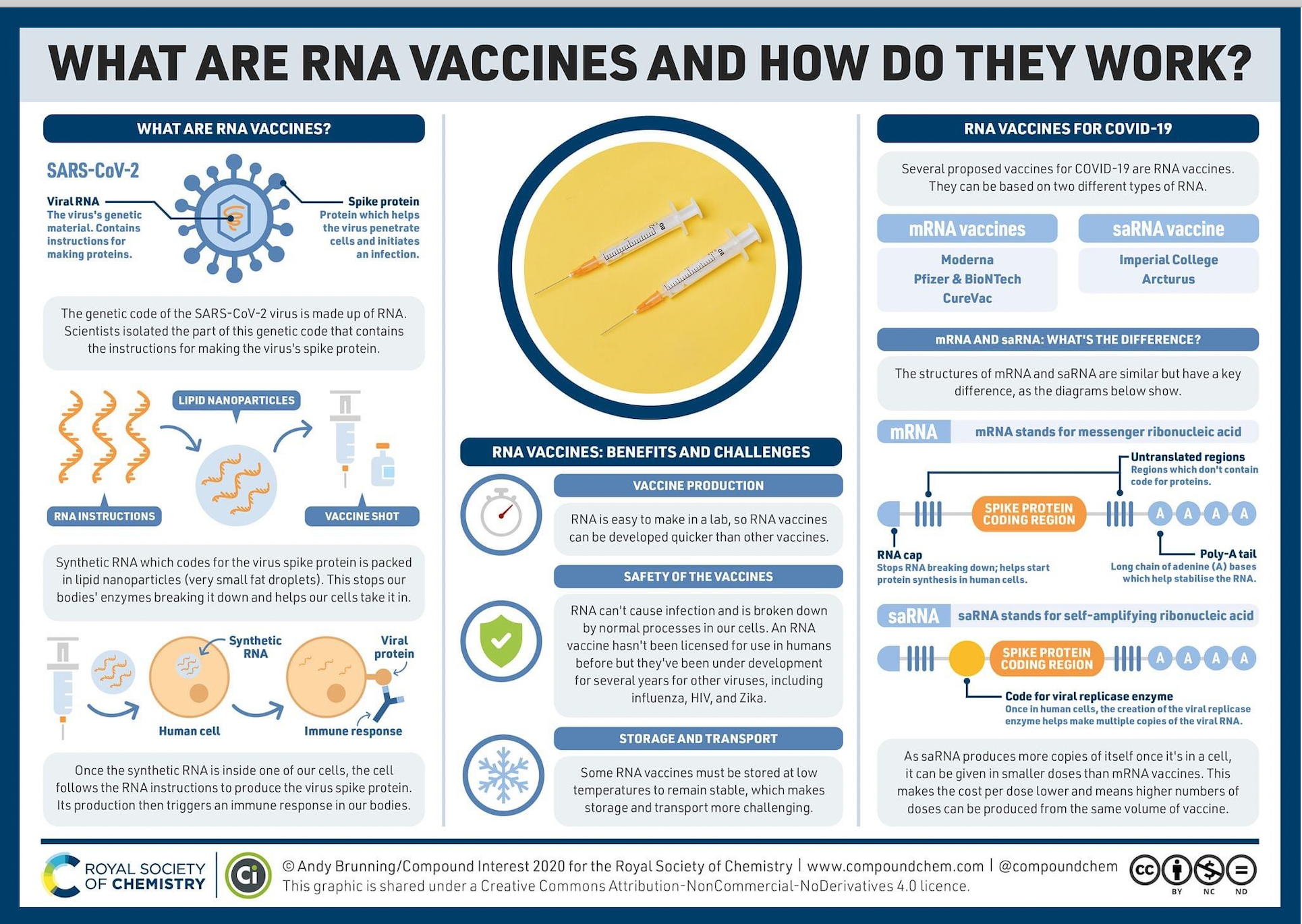
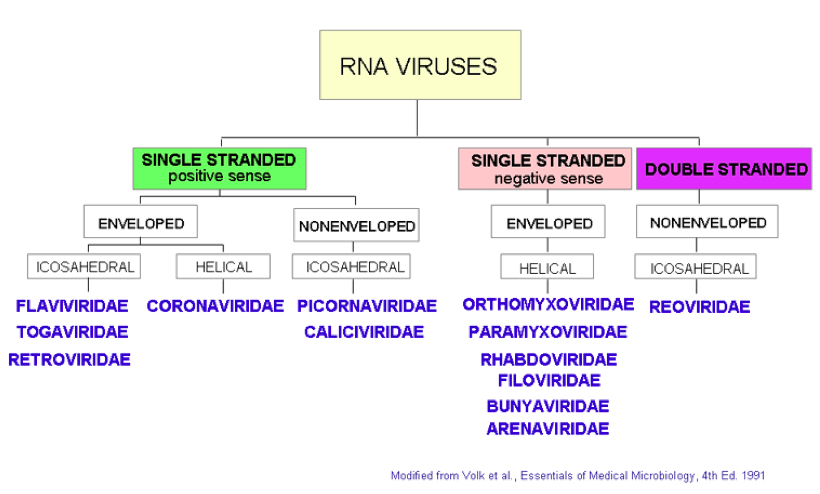
The following graphic is a good explanation of the COVID-19 vaccine. Covid-19 Vaccine is an RNA vaccine. This makes it safe since it can not cause the disease, however makes it hard to store and transport.
Physical Activity in US
November 28, 2020 1:41 pm
Physical activity in the U.S. varies based on geographic location, socioeconomic status and in comparison to other countries. It is important to know that physical activity is an important component of our well-being. However, this does not mean that going to the gym is the only way to be physically active.
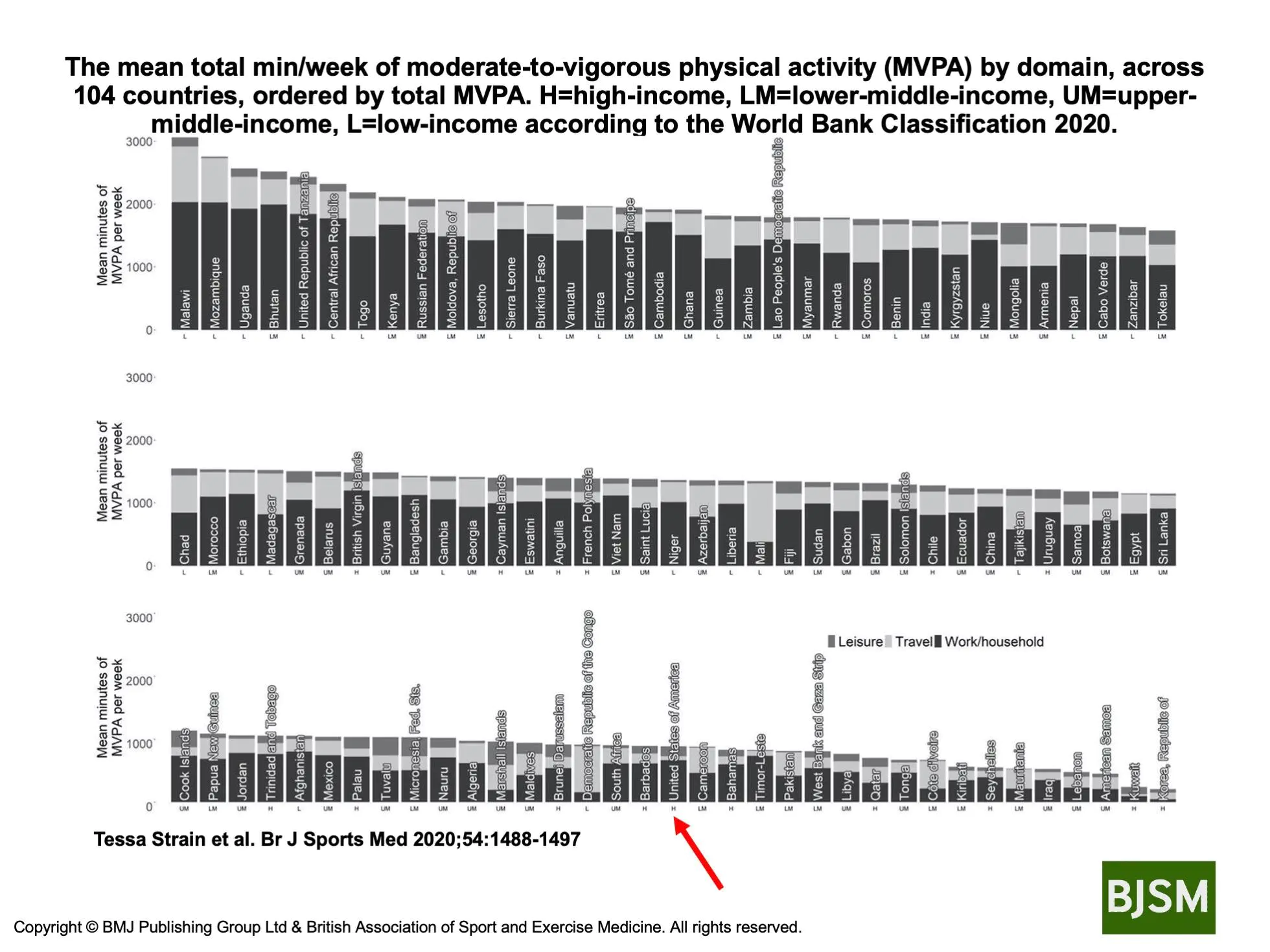
Strain et al. Shows that different populations in different countries get their activity from different sources.
His research showed that the United States population ranked as a high-income country, ranks in the lower 1/3 of the number of countries surveyed with regards to the meeting minutes of moderate-to-vigorous physical activity (MVPA) per week. This may be a contributing factor to the significant rise in obesity in the United States. Individually we should all aim to increase our moderate to vigorous activity significantly.
Activity And Your Health
November 28, 2020 1:26 pm
We should be aware that being physically active is part of being healthy. Health is a combination of being physically active, having a healthy diet are all parts of the variables that contribute to our physical and mental well-being long-term.
The restrictions and the stressors caused by COVID-19 have resulted in our inability to maintain a healthy diet and be physically active. However, we must be vigilant with maintain our activity levels to combat health issues.
It is timely that the British Medical Journal has just published an entire issue regarding the significance of activity and our health as individuals and public health worldwide.
There are a few articles that are outlined here.
Ekelund et al. Reviewed published articles and correlated the activity level and mortality. They Concluded, “Higher sedentary time is associated with higher mortality in less active individuals when measured by accelerometry. About 30–40 min of MVPA per day attenuate the association between sedentary time and risk of death, which is lower than previous estimates from self-reported data.”
Zoom Group Meeting November 24, 2020
November 24, 2020 4:40 pm

Healthcare in US
October 04, 2020 9:44 pm
The discussion has been ongoing for years about the status of healthcare in the US. Some support universal healthcare for all; some say they are against any healthcare mandate and yet demand affordable subsidized care when needed. Then, a tiny subset of the population genuinely believes in individuals’ choice and responsibility for their healthcare and well-being.
This subject of US healthcare has been studied by non-partisan groups in and outside the US at great length. The Experts at The Commonwealth Fund published a report in July 2017 which continues to be relevant today.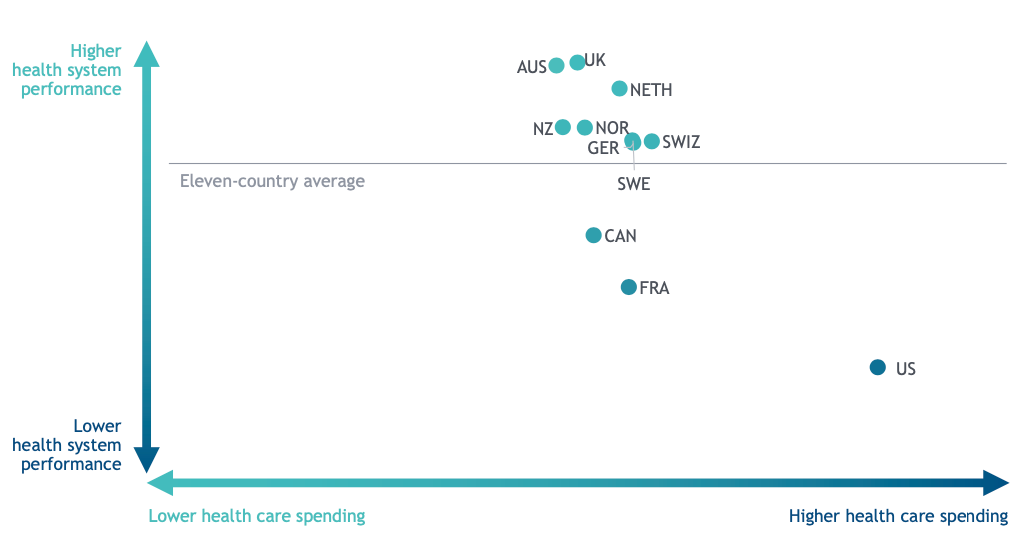
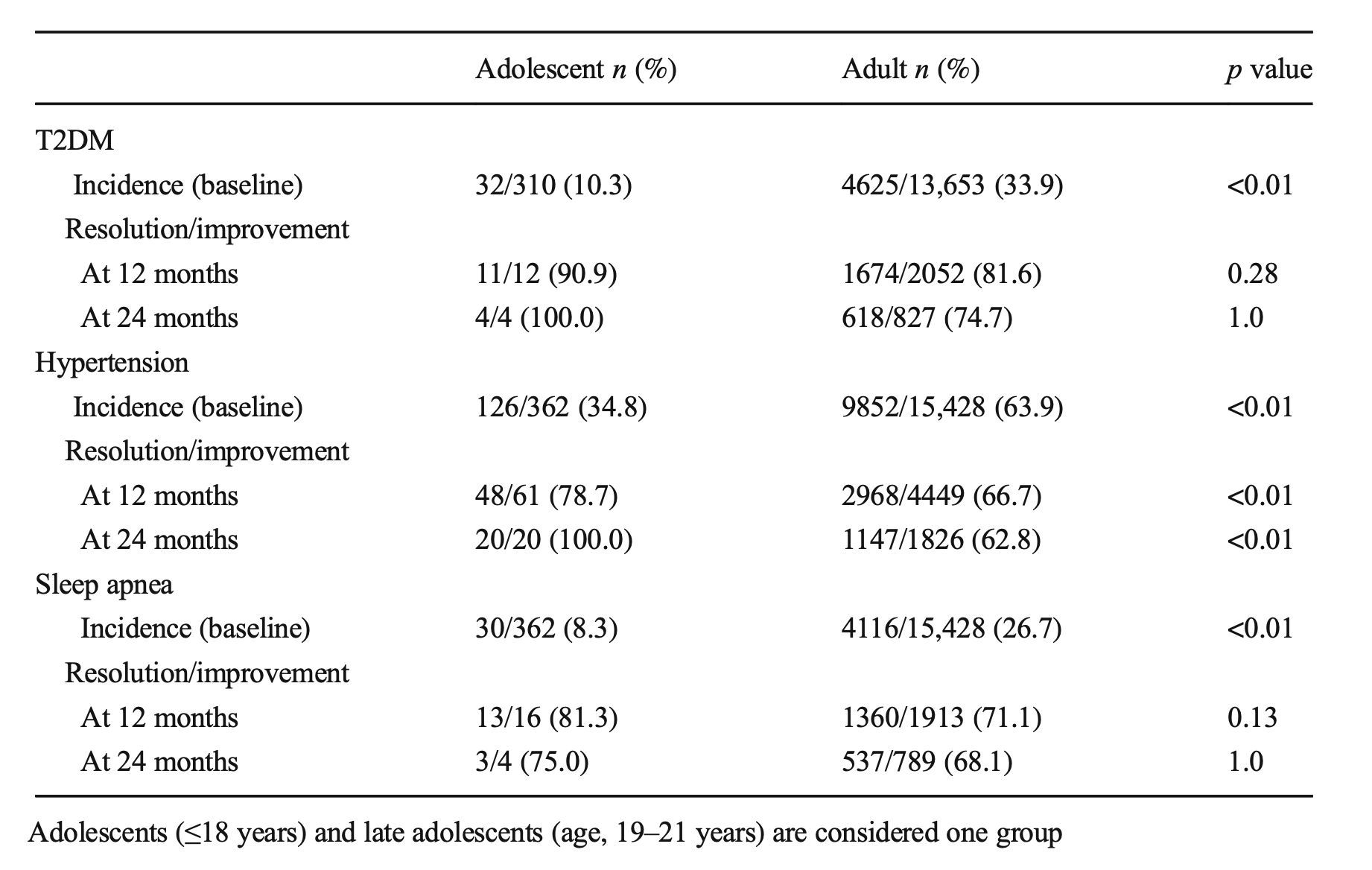
Sleeve Gastrectomy in Adolescent patients
September 23, 2020 5:44 am
Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
What is Corona Virus?
September 17, 2020 1:37 pm
Duodenal Switch Post-op One year
August 28, 2020 1:12 pm
