Oral Vitmain D
September 24, 2021 3:42 pm
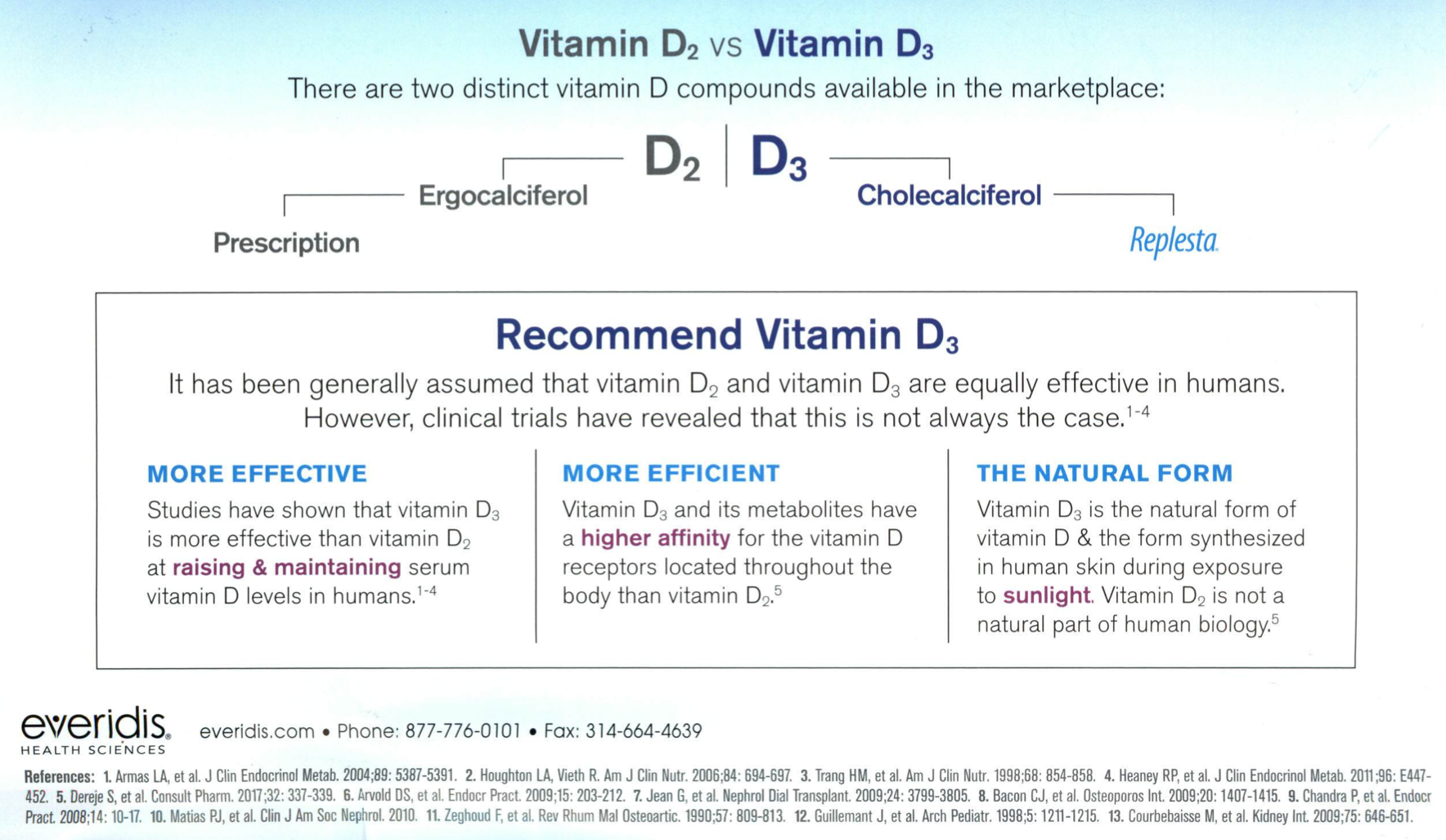
Over the Counter Vitmain D3 better than the Prescription Vitamin D2
August 30, 2021 10:41 am
COVID Vaccines
March 05, 2021 3:50 pm
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.


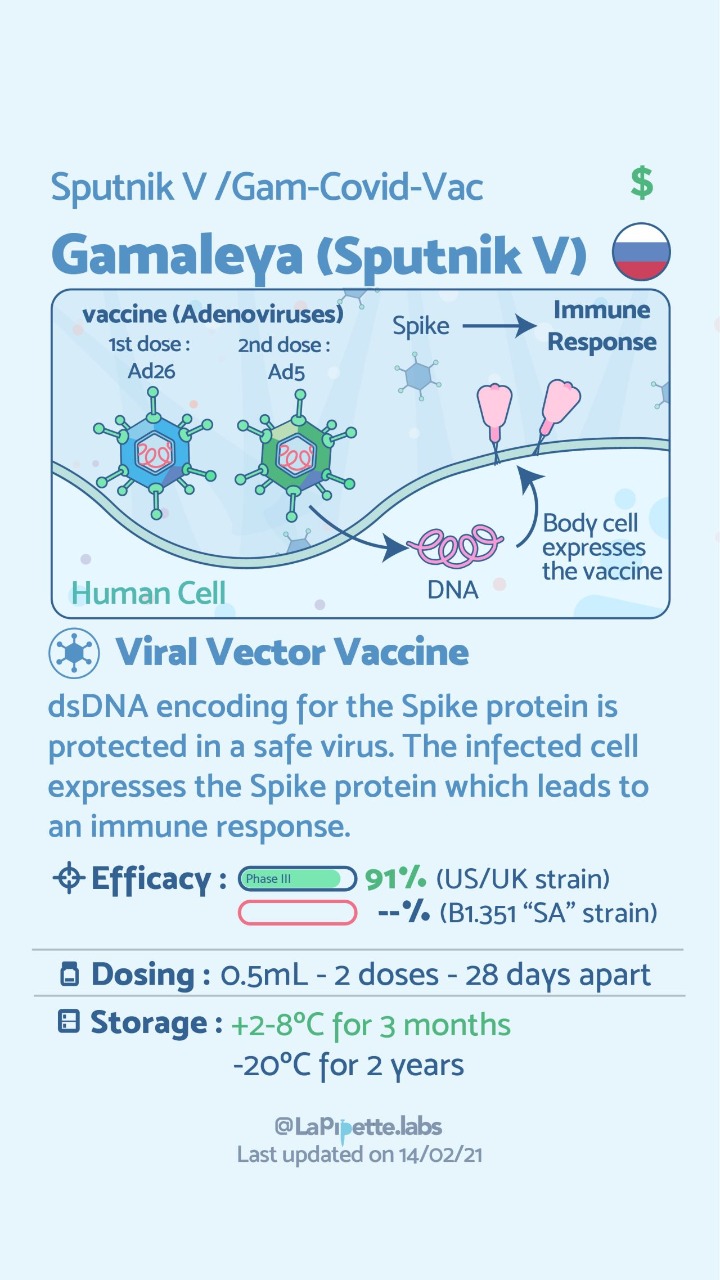

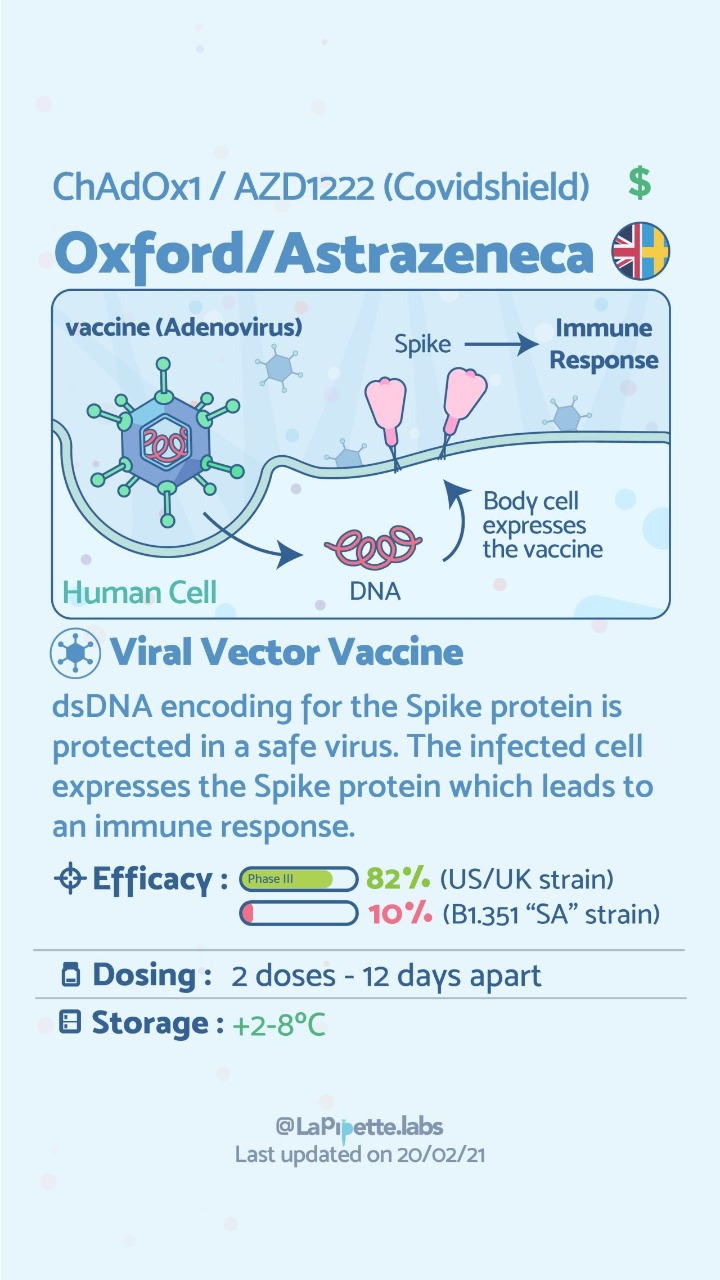
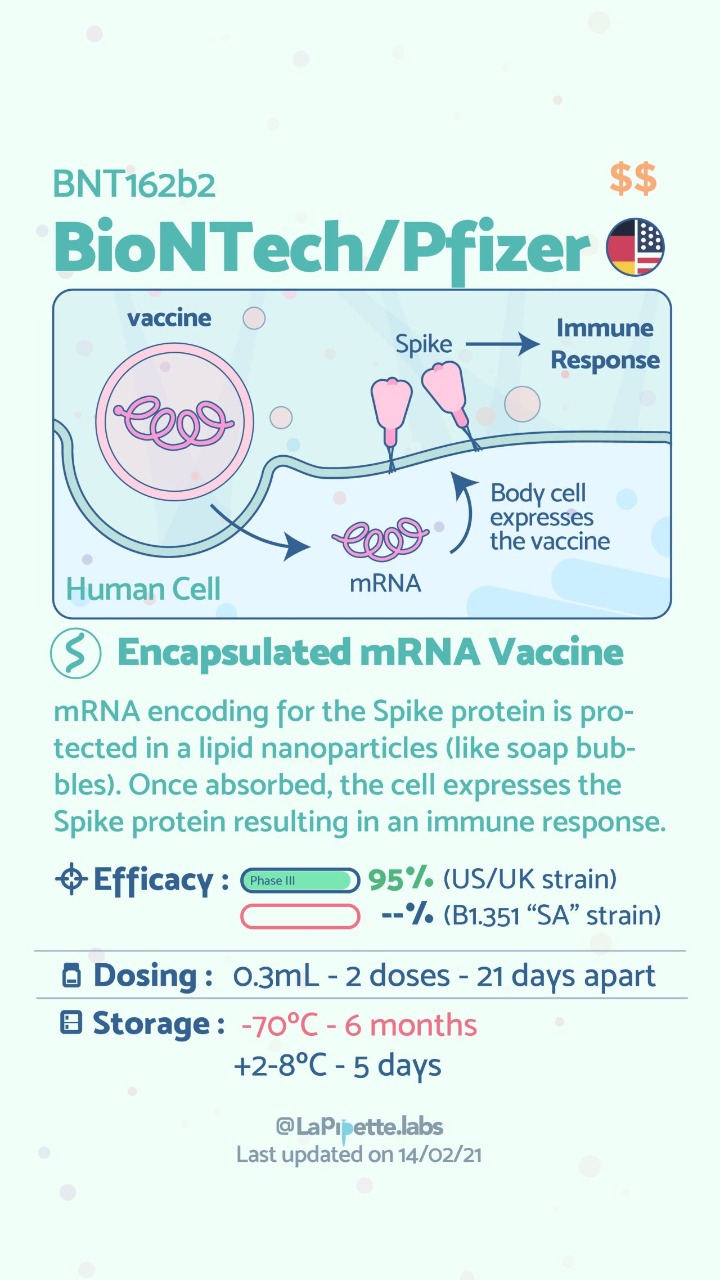
All about vaccines?
February 14, 2021 2:41 pm
Vitamin D, Immune Responce and COVID-19
January 26, 2021 6:45 pm
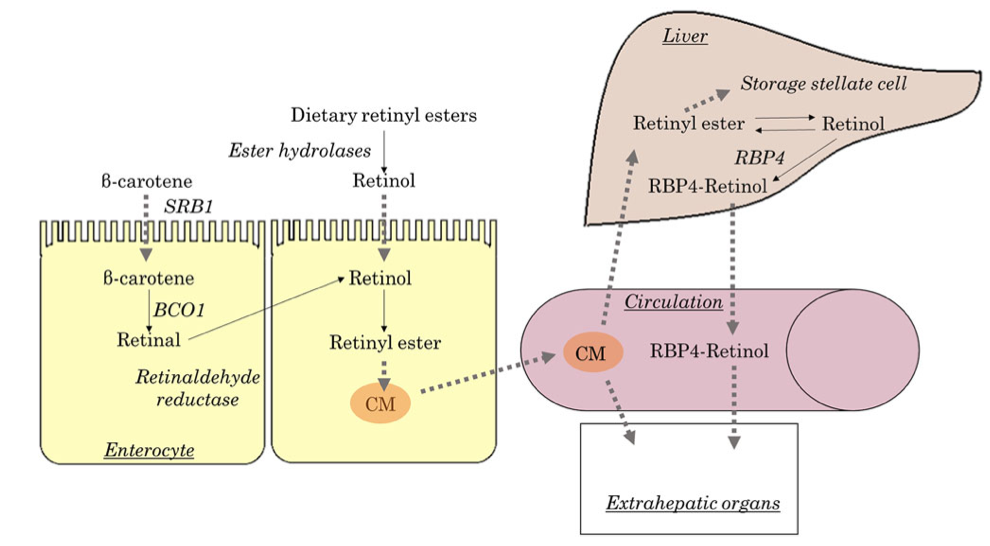
Vitamin A and Wound healing
December 21, 2020 9:37 am
Night Blindness – Vitamin A Deficiency
Nyctalopia (Night Blindness) An Early Sign of Vitamin A Deficiency with VideoA recent article discusses the types and function of vitamin A. As with the pandemic of COVID-19 continuous to stress our body and mind, we must stay vigilant with our nutritional status. Therefore, Vitamin supplements are critical in maintaining a robust immune system. For some, oral supplements are adequate; others may require injectable forms. If the oral supplements do not correct the vitamin A levels, please contact your primary care or our office to available vitamin A injections.
What’s New With the Nutrition Facts Label?
December 07, 2020 10:28 pm

Get the Facts on Serving Size
December 07, 2020 9:57 pm
The New and Improved Nutrition Facts Label – Key Changes
December 07, 2020 9:53 pm