Tag: Duodenal Switch
Surgical Treatment of Gastric Fistula
August 05, 2015 7:45 pm
Alcohol and Weight Loss Surgery Webinar May 20, 2015
July 27, 2015 7:27 am
Shared Success Story- Andrea R.
July 22, 2015 8:00 am
Since I was about 10 yrs old I have struggled with weight. I was always the chubby kid in class, and as I got older I was always the chubby friend. Being overweight didn’t affect me until I hit 220lbs at 15 years old, and as you know, kids can be mean and hurtful. At 18 years old I had my first child, during that time I dropped a little weight then ended up gaining it back and more. At the age of 19 I was sitting at 250lbs.
Fast forward 3yrs, I had my second child and once again, I lost weight just to gain back double what I lost. So now, at the age of 22 I was up to about 290lbs. Every day life became a struggle. I tried my best to stay active, but being overweight made me tired and made me feel like hiding. Over those years I tried everything from low carb diets, to diet pills, to b12 shots, and Weight Watchers; you name it, I tried it. Finally, I was fed up! I couldn’t take it anymore and I was ready to look into different options. I was 26 years old, 5ft 8inches tall, and a mother of 2 who just wanted to be active and healthy for my kids.


I decided that weight loss surgery was what I needed to do. At this point I was morbidly obese and at my highest of 326lbs. I met with Dr. Keshishian, and after going through the consultation we decided the duodenal switch would be the best option for me. On August 26th, 2013, I had my surgery weighing in at 306lbs. Dr. Keshishian is amazing! I didn’t have any complications. I was able to drink and eat small amounts normally.
Since having the surgery, just shy of the 2 year mark, I am now down to 178lbs. My life has changed so much since losing the weight! I honestly can’t describe how grateful I am that I was able to have the surgery withScreen Shot 2015-07-20 at 1.55.13 PM such an amazing Dr. and staff. Anytime I had a question or concern they were willing to hear me out and do whatever they could to assist me. Since losing the weight I am able to be the active mother I wanted to be for myself and my kids. Now I’m taking the steps needed to ensure my kids learn healthy eating habits and helping them understand how important exercise is.
Andrea R.
Informed Surgical Consent
July 18, 2015 9:39 pm
Surgical informed consent is the document that summarizes the discussion that has been carried out between the treating physician and the patient. It also outlines the expectations as well as the potential complications of the treatment being proposed.
An informed consent should mean that the patient is absolutely clear as to the procedure agreed upon and that is reflected on the consent. No abbreviations are allowed on the consent forms. Clearly, there are instances when a physician or surgeon providing service may have to deviate from the proposed plan and agreed upon procedure on the consent because of unexpected findings in the operating room.
Any patient undergoing surgery should be acutely aware of the terminology and the language used. With regards to weight loss surgical procedures, RNY and GB is not acceptable because they are both abbreviations.
Duodenal Switch is a distinct well described procedure with its unique identifiable code (43845 for open procedure) that is recognized by hospitals, insurance companies and the surgical societies.
Duodenal Switch operation is not SADI, SIPS nor a loop Duodenal switch. Any attempt to interchanges these terms or operations is inaccurate the say the least.


A surgical informed consent is signed by the patient ( or the guardian) and the treating physician. This document however is reviewed and confirmed by all those involved in the patient’s care delivered in the hospital. The consent is reviewed by the admission staff when taking the patient for surgery, preoperative nursing and administrative staff, operating room circulating nurse as well as the anesthesia staff. One step most patients may not be aware is initiated after the general anesthesia is induced. The operating room staff, anesthesia staff and the operating physician all go through a set of checklist known as “Time out”.
“Time out” involves confirming the patient’s identification as well as the proposed procedure as the patient had discussed with the staff and confirming the consent.
It is imperative that a patient have complete understanding of their surgical options available to them and critical that they have full knowledge of the type of surgical procedure that has been consented to and performed.
Iron Deficiency & Anemia July 15, 2015 Webinar Recording
July 16, 2015 1:52 pm
Vena Cava Filter
July 06, 2015 7:09 am
Example of a Vena Cava Filter Video:
Shared Success- Whitney a RNY to DS revision
June 09, 2015 7:43 am
I was always the big girl, pleasingly plump, chubby. I was put on my first diet at age 12. By the time I graduated High School I had yo-yoed up to 200 pounds at College graduation I was up to close to 300 pounds. In 2002 I had RNY Gastric Bypass surgery. I was 39 and weighted 280 pounds. I was told it was the Gold Standard. The Band was still considered experimental and the Duodenal Switch was never mentioned as an option. In fact, I did not even know it existed.
I lost 110 pounds and was considered a WLS success. I did not have any food restrictions and I felt great and maintained the loss for five years. Then I started to slowly gain weight. In little under 5 years I gained 70 pounds. I developed Dumping Syndrome and my Stoma was stretched out. I joined Weight Watchers and lost 5 pounds in a year. Nothing worked. I developed ulcers, osteoarthritis, planter fasciitis and could barley walk a couple of blocks without pain. I was miserable. I felt like a failure
In 2012 started to research surgical options. A local surgeon wanted to “revamp” my already tiny stomach, put a band around my stoma, and “clean up my intestines”. I asked about revision to Duodenal Switch and was strongly discouraged, but I wasn’t going to settle because that was what he was only capable of doing.
")
")
I wanted the best. I wanted long term success. So I travelled from Northern CA to Southern CA for a consult with Dr. Keshishian. The only choice for me was to revise to DS. In December of 2012, I had revision surgery of my RNY to Duodenal Switch. One week after surgery, still in the hospital, I went in for a second surgery. Dr. Keshishian found a small leak. I spent an additional two weeks in the hospital. My experience was not the norm and a leak can happen in any surgery involving the stomach.
Recovery was slow but steady. The first 2 weeks Dr. Keshishian called me every three days to make sure I was doing ok. I still have his cell number in my phone. I was back to work 14 weeks after surgery. I could have gone back sooner.
Over the past year I have lost 115 pounds. My BMI is 20, and I feel great. I have my life back. All pre-op issues have been resolved and I am going to start training for a 5K.
My advice for anyone contemplating Weight Loss Surgery is to research all of the options available. Do not settle for a substandard surgery. Get a second or even third opinion. It’s not a decision to be taken lightly. It’s your life fight for it!
Whitney B.
Neuromuscular Disease After Weight Loss Surgery
June 08, 2015 11:30 am
Weight loss surgical procedures may result in varying degrees of nutritional deficiencies. Some of these nutritional deficiencies may cause neuromuscular disease if left untreated, these include vitamins, minerals, and protein. The long-term effect of these deficiencies may presents as neuromuscular conditions including, weakness, numbness, confusion and all others if not-diagnosed and untreated. It is important to note that all weight loss surgical procedures require lifetime vitamin, mineral supplements and protein monitoring and possible supplements.
The table below outlines some of the specific neurological and neuromuscular disease complications following bariatric surgery. The most common deficiencies seen with the duodenal switch operation are fat soluble vitamin deficiencies. These include, Vitamin A, D, E and K. Duodenal Switch patients need oral supplements of Dry “Water Miscible” type of Vitamin A, D, E, and K based on their laboratory studies and needs.


The neurological deficiencies are manifested much more frequently with the Gastric Bypass than the duodenal switch operation. The most common nutritional deficients are that of B1, B12, Folate deficiencies that are common in Gastric Bypass. A list of possible neurologic deficiencies and there associated symptoms were summarized by Becker (2012). Another article with Nutritional Neuropathies.
Nutritional deficiencies are seen in a number of illnesses including weight loss surgery patients.
Coping Skills after Bariatric Surgery
June 02, 2015 7:23 am
For many people, food can become a coping mechanism and a way to self sooth or comfort themselves. After weight loss surgery the ability to use food in this manner is disrupted due to the smaller portions and in some cases food intolerances. Developing alternative and healthy coping skills is an imperative step after weigh loss surgery.
Obesity is a multifactorial process that has many contributing aspects. Although, obesity is not entirely the result of poor eating behavior, and lack of exercise. After weight loss surgery, we should appreciate the importance of healthy dietary choices; being sure that volume and frequency is not driven by emotion or emotional eating.
The mental aspect of weight loss surgery should not be ignored. Developing healthy coping skills can be a large part of dealing with the changes that take place. Some people go through a mourning period for the loss of the foods that once gave them comfort, made them part of a group, or the feeling of their best friend. In some cases, there may be a need to seek the assistance of a mental health care provider to be able to work through some of the issues and feelings. Never hesitate or be afraid of contact a mental health care professional.
Learning and practicing effective coping/soothing techniques can be started prior to weight loss surgery. The following are some coping skills that can be effective for some to adopt into their daily lives.


1. Nature – Get out into the great outdoors and into the sunlight. The sounds and sights of nature have a way of energizing the body and calming the mind. Sunlight is excellent for increasing Vitamin D levels which can help elevate mood and general well being.
2. Exercise – The mental and physical effects of exercise are paramount after weight loss surgery. The natural chemical release from exercise is a calming effect and gives a sense of well-being. In addition, the physical aspects of increase weight loss and change in body contour have positive mental and emotional effects.
3. Music- There are many research articles regarding the positive effects on both metal and physical aspects of music. Music has a way of soothing or energizing the soul. Turn up loud or keep it soft. Sing along. Dance it out if you need to.
4. Journaling – We always suggest to people prior to weight loss surgery to start journaling. It can give you perspective when you look back at entries. We also suggest to journal body measurements, pictures, and weights so that you might look back at how far you’ve come from your starting point.
5. Mindfulness – Using all five sense to experience life and food. Take your time to take everything in and experience the full effect. Be present in all life experiences. Ask yourself: Am I enjoying this? Does this feel like what I need? Is this getting me to where I want to be? Is this healthy for me?
6. Support groups of peers- There is nothing like having a group of people who have been there or know exactly how you may be feeling to be able to talk, share or vent. There are so many support groups that can be taken advantage of in either face to face or cyber groups.
7. Treat yourself- Treat yourself and practice self-care by doing something that you find relaxing, gratifying or energizing. Massage, manicure, an outfit, shoes, an outing, or a class.
8. Distraction- Hobbies, new skills, reading, games, bubble bath, or anything that get you out of the same mental spot can help with calming and soothing.
9. Talking- There is great value in having a close friend or trusted therapist to be a sounding board and give you an opportunity to unload some of the challenges you’ve been carrying.
Changing habits and coping skills takes practice and patience. It is not something that is easily changed over night. Focus on small steps, goals and achievements. Give yourself time and credit for the accomplishments that you’ve made. Always look at how far you have come and the positive lifestyle changes you’ve made. There may be set backs but don’t beat yourself up about it, move on and continue to take steps toward your goal.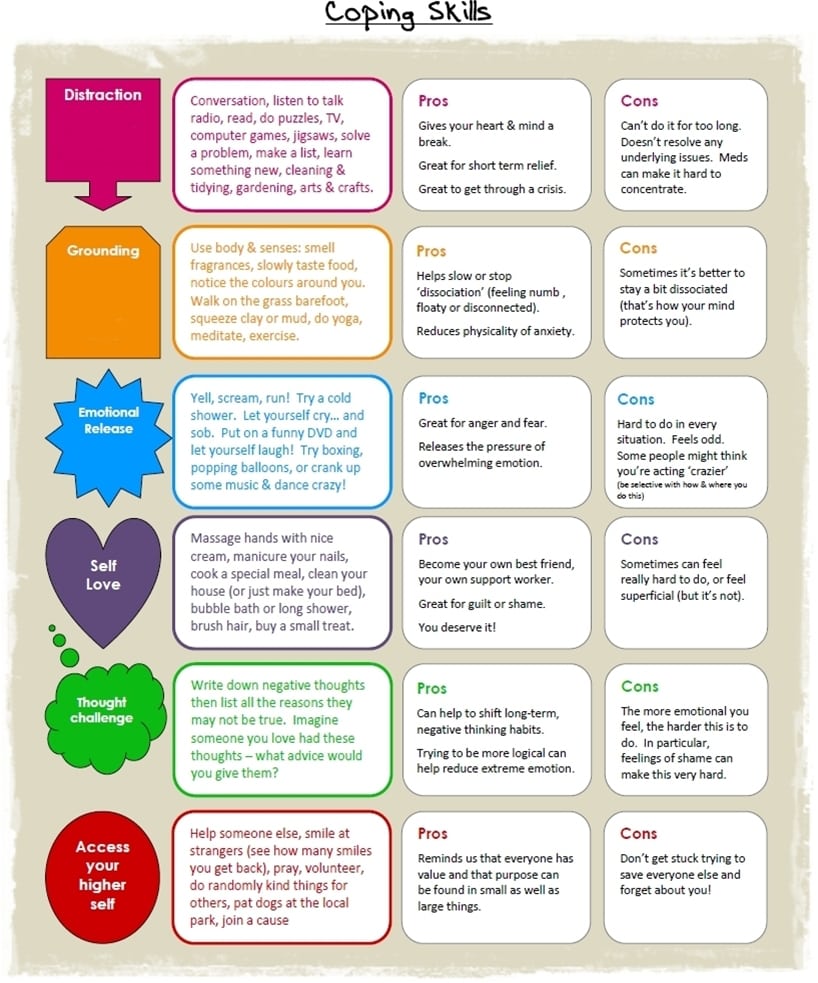
https://www.counselorlady.com
Duodenal Switch and Fat in The Diet
May 21, 2015 12:35 pm
When I perform the duodenal switch operation, the common channel is a percentage of the total small bowel length and I also account for the patient’s metabolic rate. Two individuals with a BMI of 50, should not have the same common channel. If we compare two patients, one of them is a 20 years old male who is 6’2″ and the second patient is a 60 year old female who is 5’4″, we can see how this applies. These two patients have very different metabolic needs and requirements. When the Duodenal Switch is performed in this fashion, the common channel based on a percentage of total small bowel length and metabolic needs, the patients post op diet works best when it is a well balanced, protein based diet. The basic principals are : Hydration (water), Protein and Everything else, low carb, avoid artificial sweeteners, avoid carbonated drinks, have frequent smaller meals and avoid processed food. Listen to you body as to what it tolerates and what it doesn’t. This is what I recommend for my patients.
I am not aware of any scientific evidence that proves any benefit to excessive amounts of fat for DS patients who have had their length of the common and alimentary bowels based as a percentage of the total length.
My recommendation are to have a well balanced high protein diet. I do not recommend a low fat diet, except in the healing phase after surgery. However, there is no reason to consume excessive amounts of fat long term.
High fat diet is used to facilitate bowel movements for some patients who have constipation. It may be prudent to try and identify what may be causing the constipation and correct or eliminate them before one resorts to a very high fat diet as a “treatment” for constipation after Duodenal Switch. The possible causes for constipation after duodenal switch may be metabolic-organic (where some patients have infrequent bowel movements before DS, hypothyroidism), length of the common and the Alimentary channels and medications (pain meds, narcotics, antidepressants).
In addition, Medium Chain Fatty Acids do not require bile salts to be absorbed and are directly absorbed into the Portal Vein in the liver. Medium Chain Fatty Acids are not malabsorbed post Duodenal Switch. Medium Chain Fatty Acids included Caproic acid, Caprylic acid, Capric acid, and Lauric acid. Commonly found in varying amounts within coconut oil and palm oil. MCT supplement is made with Medium Chain Fatty Acids.
In summary, I recommend that Duodenal Switch patients who have had surgery with our practice have a high protein balanced diet. I do not recommend avoiding fat, or going on a low fat diet. I am not sure if there a reason to consume excessive amount of fat, which may in fact have unexpected metabolic and nutrient consequences.
Every patient, as their weight stabilizes, will find what works and what does not work for them. Some patients will tolerate a higher fat intake and other will not be able to tolerate higher fat intake.