Category: Dumping syndrome
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
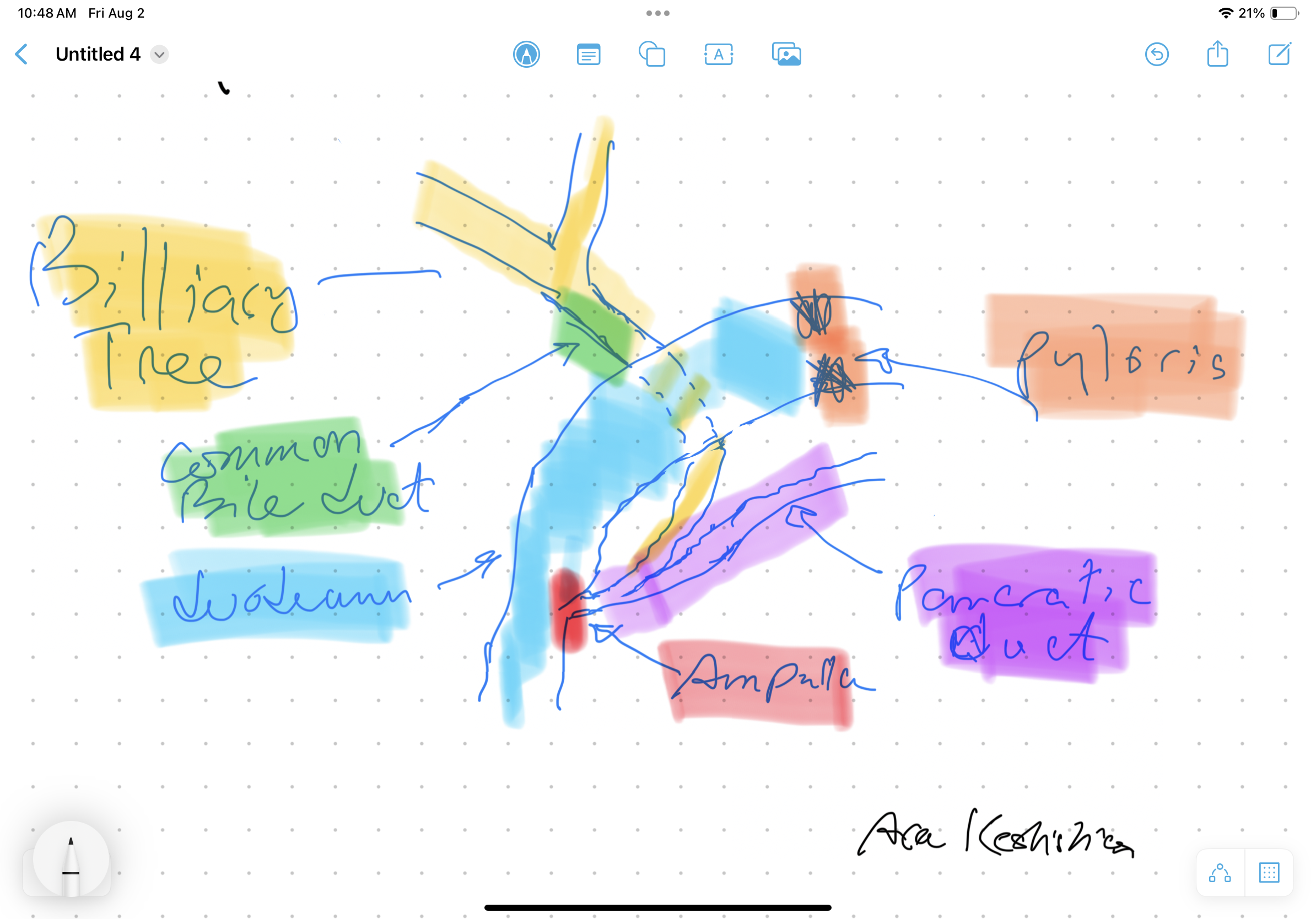
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

Shared Success Story: Kerry F. had a Gastric Bypass revision to Duodenal Switch
May 27, 2014 2:12 pm
Revising from RNY to Duodenal Switch
Spending my entire life overweight, I thought I found the answer when I had my RNY gastric bypass surgery in July 2001 at the age of 24. I was 354 lbs. at 5’9 and after RNY gastric bypass lost down to my lowest weight of 192 lbs. I kept that weight off for 6 years.

Then due to my previous surgeons lack of information about vitamins (I needed an iron transfusion in 2004 due to iron deficiency anemia and malnutrition) and my ignorance of proper eating I ended up gaining 150 lbs. back in just 3 years from my intestines reabsorbing and a stretched pouch. I felt like a complete failure, embarrassed and angry. I turned to a website about putting Lap Band over bypass, a new procedure. While investigating, Dr. Keshishian I found out about revising to Duodenal Switch (DS) and how it can help lose the weight and keep it off through adherence of diet and vitamins.
I feel amazing at the age of 37 and thank Dr. Keshishian for giving my life back to me
AGAIN, always telling me from day one that I was NOT a failure – the RNY was. He also said to believe in myself, follow the plan and be proud of my accomplishments. And I am!!! My advice to all – do your research, know ALL of your options, make the best decision for you and if you want a DS revision go with one of the BEST, Dr. Keshishian. He won’t steer you wrong! I’m living proof!!!

Revision or Reversal of the Duodenal Switch
September 08, 2012 7:00 pm
A significant portion of my practice involves the revision of the Gastric bypass and Adjustable Gastric Banding procedures to the Duodenal Switch operation. The re-operations are necessary to correct the complications that have been caused by these procedures. There are also instances of required revisions due to inadequate weight loss or weight regain. Our website contains detailed information regarding reasons for revision and the reversal of weight loss surgical procedures. I think it is important to mention that these complications are very common and almost never have anything to do with the patient’s behavior.
Duodenal switch operations may also require reversal or revision. The general reasons for a revision or reversal of the Duodenal Switch is the same as for all weight loss surgical procedures and include a variety of reasons. The reversal or revision of the Duodenal Switch operation is one of the simplest revision surgeries that I perform.
Let’s review a few facts about Duodenal switch.


The Duodenal Switch procedures has two components:
1.) The sleeve gastrectomy
2.) The separation of the biliopancreatic secretions from the food to limit its absorptions.
Clearly, the portion of the stomach that has been removed cannot be reintroduced to the abdominal cavity. The second part of the operation can, however, be easily “undone.
The assumption is that the bowel needs to be divided again and re-anastomosed to reconstitute its continuity. This revision or reversal of the Duodenal Switch operation is done by simply creating a new connection between a new anastomosis, located between the biliopancreatic limb, and the alimentary limb.
If a complete reversal is needed, then the connection is made just distal to the ligament of Treitz. Ligament of Treitz is the transition point between the duodenum and Jejunum. This single anastomosis is safe and simple to perform and does not involve removing the previous staple lines.
If a partial revision is needed, or the common channel needs to be lengthened, then the anastomosis is made further proximal to the junction of both the alimentary limb and the biliopancreatic limb, but distal to the ligament of Treitz to allow for increased absorption of the calories and nutrientsIn my opinion, the revision and reversal of the Duodenal Switch operation is, from a technical perspective, the simplest of all revisional weight loss surgical procedures.
In my opinion, the revision and reversal of the Duodenal Switch operation is, from a technical perspective, the simplest of all revisional weight loss surgical procedures.
Does duodenal switch correct dumping syndrome and the hypoglycemic complication of The RNY-gastric bypass, and it variations? A patient’s story
May 20, 2011 7:13 pm
On 10/28/2009 I had a variation of the RNY gastric bypass known as the Fobi pouch. I lost over 270 pounds, but I had debilitating complications of dumping syndrome, reactive hypoglycemia, acid reflux and vomiting.
My entire day was pretty much controlled by dumping syndrome. Due to the hypoglycemic episodes that resulted from dumping syndrome, I was constantly in a binge cycle, because I constantly needed to stabilize my blood sugar. I would eat breakfast and need to lay down. Once I started having hypoglycemia, I would get up and splurge on carbohydrates.
Note that my dumping syndrome was not caused by poor food choices. I only splurged off carbohydrates in a desperate attempt to quickly get my glucose levels up. This did work, but it lead me to dumping syndrome again. I then had another episode of hypoglycemia, which lead to more binging which resulted in more dumping, more binging and weight gain. Here is a diagram of the cycle I was constantly in:
Eat –> dump –>hypoglycemia –> binge –>redump –> more hypoglycemia –> binge –> dump
This was a constant cycle I was in, and as you can see here, my entire life became controlled by dumping syndrome, and it eventually caused me to become disabled. I am a full time student and was not able to go to school in this state. I would eat lunch and then go to class only to start dumping ten minutes into lecture, and I ended up dropping my classes for the semester.
I went to my bypass surgeon and told him of the problems I was having, and he told me that I was anorexic. I was also told that it was “…all in my head.”
After doing much research, I consulted with Dr. Keshishian. I handed him a list with the problems I was having and asked if revision to the duodenal switch would resolve these problems. Dr. Keshishian drew out a diagram of the anatomy of my surgery and showed me exactly why I was having these complications. I remember him saying, “There is a physiological explanation for why you are having these problems. It is not in your head. Yes, revision will resolve these complications.”
I had my revision on 4/11/2011, and all the complications I had with my bypass have been resolved, and I have had no complications with my duodenal switch. Now that my pylorus is working again, I can eat without becoming ill. I have now gone back to school, work, and have resumed back to a normal life.
YG