Tag: bile reflux
Bile Reflux Gastritis
May 19, 2026 4:13 pm
Hello, it’s best to clarify a few points:
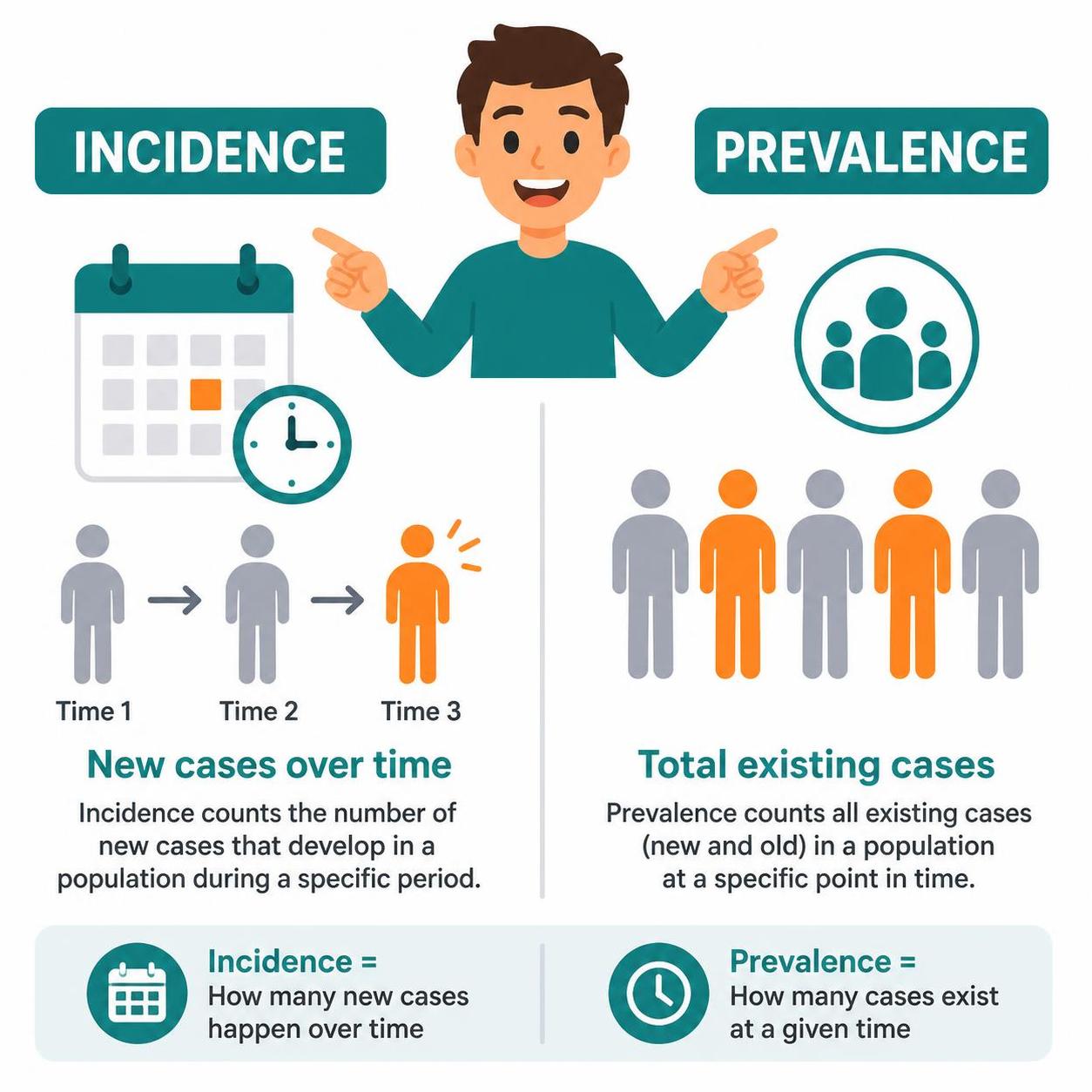
- The difference between prevalence and incidence.
- Incidence means new cases over
- Prevalence refers to existing cases at any time
- The difference between causation, coexistence, and correlation
- Causation refers to a condition causing an effect.
- Coincidence refers to two conditions present together at the same time, with neither causing the other.
- Correlation refers to two conditions that may occur together, with no causation.
- Study size refers to the research data on which the information is based. The larger the population size studied, the better the sample data and the more conclusive the results.
- Confounding factors.
Sphincter of Oddi Dysfunction
April 26, 2026 8:43 am
Description:
Sphincter of Oddi Dysfunction (SOD) is a clinical syndrome characterized by biliary/ pancreatic pain from abnormal function or obstruction of the.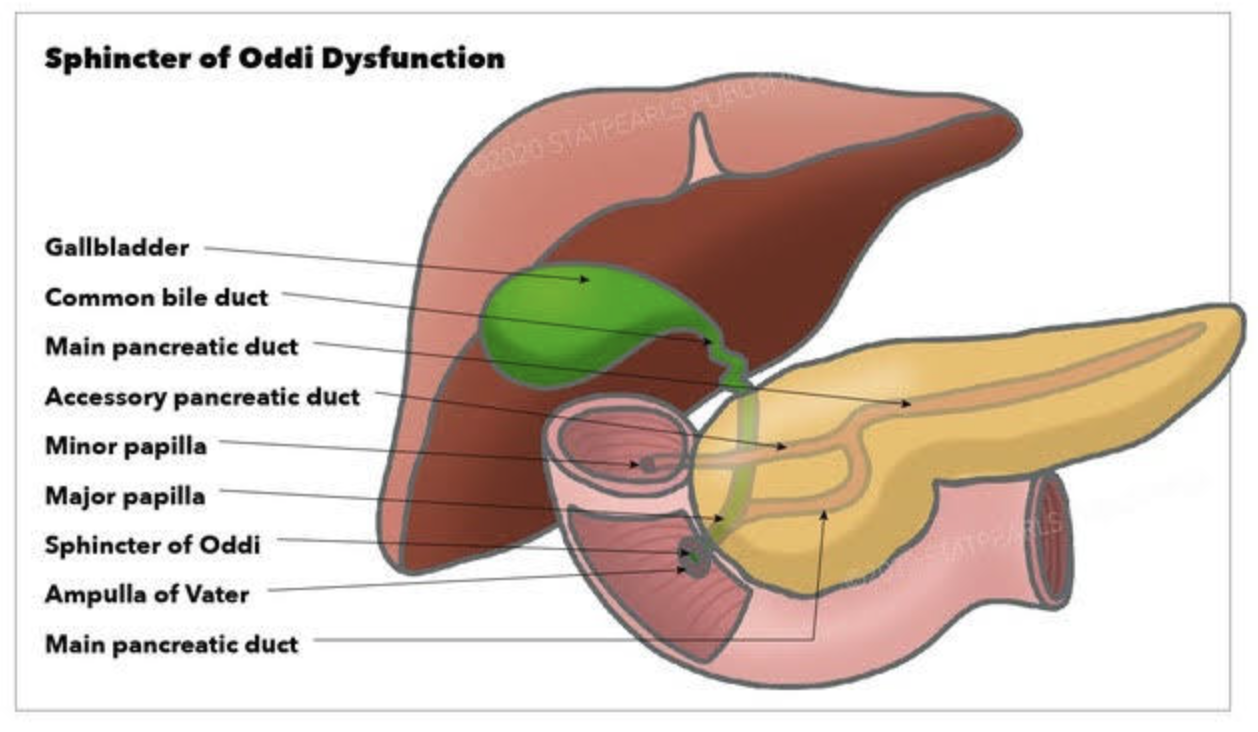
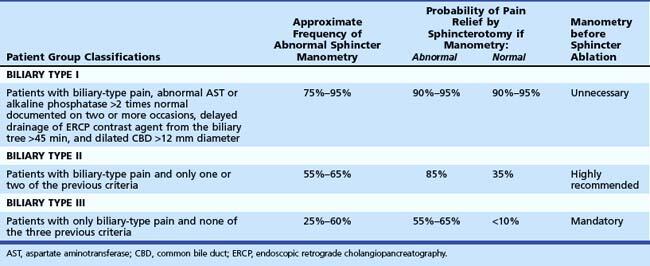
Diagnostic and classification
- The SOD spectrum includes biliary, pancreatic, or combined sphincter dysfunction, with symptoms driven by dyskinesia or mechanical obstruction. The term SOD encompasses both functional motility disorders (biliary or pancreatic sphincter dysfunction) and mechanical obstructions such as papillary stenosis.
- SOM has been considered the gold standard for diagnosing elevated basal sphincter pressure. It is invasive and carries complications, including pancreatitis. SOM can also not be done in those who have had gastric bypass or duodenal switch operations. Sphincterotomy outcome is not uniform. Consequently, many centers have moved toward empiric endoscopic therapy for appropriately selected patients and toward noninvasive or less invasive diagnostic approaches for others.
Treatment approaches
- Endoscopic biliary sphincterotomy (EST) is the most established nonpharmacologic treatment for biliary SOD, particularly in type I and many type II patients with objective ductal dilation and/or enzyme elevation.
- In type II SOD, outcomes after EST correlate with objective evidence of obstruction or sphincter hypertension on SOM. Empiric sphincterotomy without manometry is controversial.
- Type III SOD has emerged as predominantly functional pain rather than a mechanical obstacle. Alternative management emphasizes risk stratification, noninvasive strategies, and multidisciplinary approaches.
- Medical and non-sphincterotomy options (calcium-channel blockers, nitrates, antidepressants, and lifestyle modifications) have been discussed as potential adjuncts or alternatives.
Summary
- SOD is a multifactorial biliary and pancreatic sphincter disorder with a spectrum from mechanical obstruction to pure dyskinesia. Type I and II retain treatment relevance, particularly EST for biliary obstruction. Type II management requires clear identification of the cause.
- SOM is a diagnostic tool with significant limitations.
- Endoscopic sphincterotomy offers meaningful symptom relief in type I and select type II with objective obstruction. It carries a risk of complications, including pancreatitis; risk mitigation strategies are integral to practice. In type III SOD, sphincterotomy generally has limited benefit, necessitating a move toward noninvasive management and careful patient counseling. Patients post- gastric bypass, or duodenal switch, can not have ERCP or SOM done.
Bile Reflux Gastritis and Cholecystectomy
May 21, 2025 2:41 pm
Bile reflux gastritis is not a the result of the cholecystectomy but may be seen in a subset of patient with other confounding conditions. Bile is produced in the liver and stored in the gallbladder. In response to high fat and protein in the stomach, the gallbladder contracts to ” squeeze” the bile stored in the gallbladder into the small bowel to help absorb the fat and protein.

With the gallbladder removed, the bile produced by the liver cannot be stored and goes directly to the small bowel via the biliary tree.

It is possible and likely that some of the bile will find its way back to the stomach. In some patients, due to compounding circumstances, the bile may collect and cause gastritis. We need to dissect this a little for it to make sense.
- Not every patient after cholecystectomy will have bile in their stomach.
- Not every patient with bile in the stomach has gastritis.
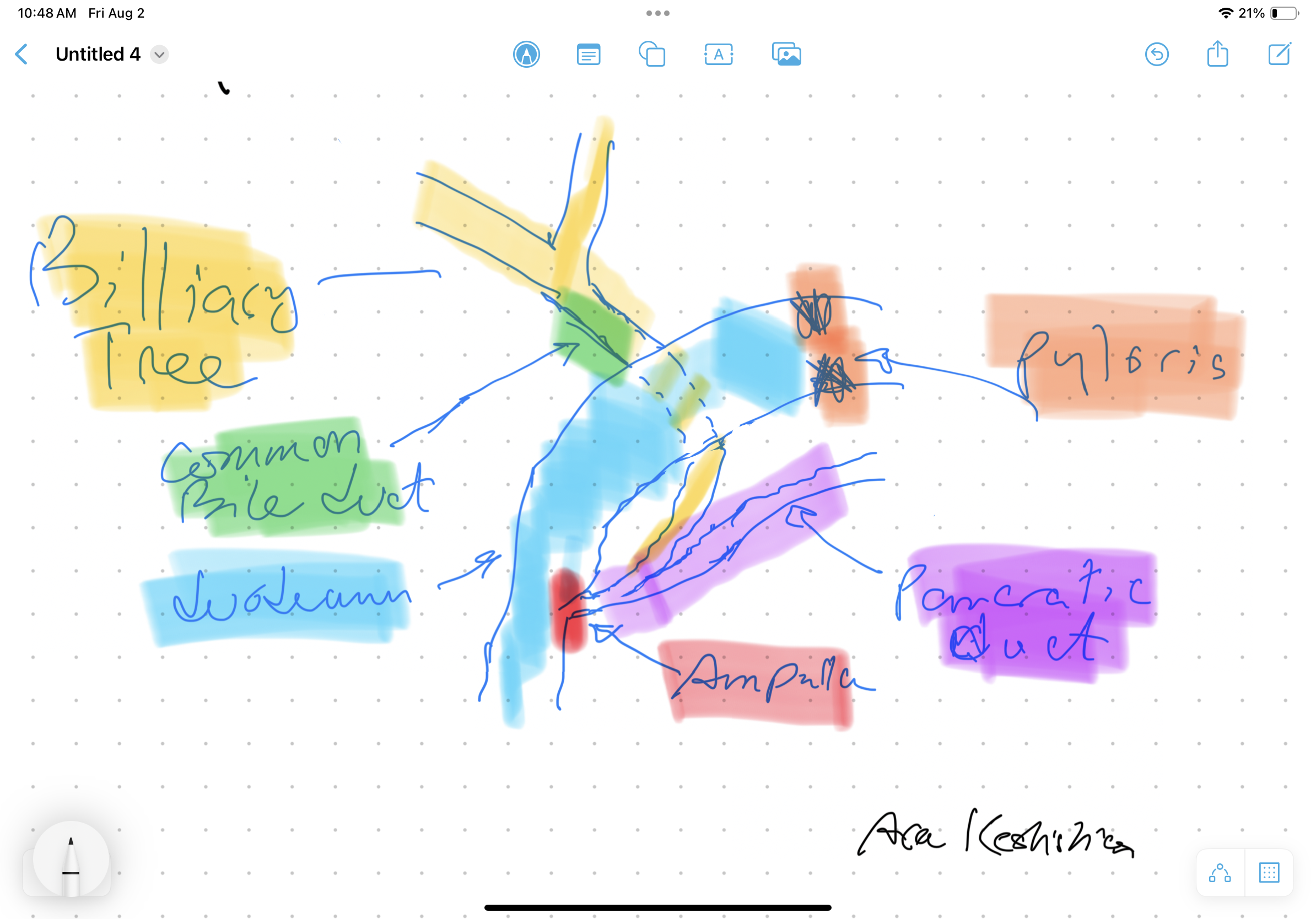
To appreciate this, let’s remember that for bile to get from the small bowel to the stomach, it needs to:
- Go upstream, against the peristalsis of the small bowel, and do not be washed down by the flow of the gastric
- juices coming out of the stomach.
- Go through the pyloric valve.
- If it reaches the stomach, the acid in the stomach does not neutralize it, causing gastritis.

As I’m sure we all appreciate, other contributing factors besides cholecystectomy may cause bile reflux and bile reflux gastritis. This is why it’s also emphasized that bile in the stomach alone does not confirm biliary reflux gastritis. It is also why we always state that bile reflux gastritis is a disease of exclusion, where other conditions such as gastroparesis, acid reflux, and hiatal hernia (regardless of size, as some patients are unfortunately told that since the hernia is small it does not need to be fixed, which is incorrect) must be considered. Further information on Bile Reflux.
Billary Diversion is the only definitive surgical procedure for Bile Reflux Gastritis.
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary tract flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or a tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis is reserved for cases with no alternatives.

Billroth I & II, SIPS, SADI, Loop
July 27, 2015 1:30 pm
In 1881, Dr. Theodore Billroth performed the first successful gastrectomy for pyloric tumor. He removed the distal part of the stomach and tumor of the pyloric region and reconnected the distal end of the transected stomach directly to the segment of the duodenum. This was later renamed as Billroth I procedure. In Billroth I the anastomosis allows the food pathway to stay in the same directional flow with the exception of pyloric valve having been removed. There is, however, increased incidence of bile reflux with the pyloric value removal.






There are incidences where the resected segment is so large that the proximal stomach and the distal duodenal can not be mobilized and brought close to each other to be able to create the Billroth-I anastomosis. Larger resection, where the Billroth I could not be completed Dr. Billroth in 1885 created a procedure call the Billroth II. The Billroth II was performed when the tumor was very large and the continuity of the GI track was created by a loop gastrojejunostomy. This procedure was named Billroth II.
In the Billroth II the bile flow from the small bowel flows toward the stomach, and this results in a much higher incidence of Bile reflux and its associated complication.
The lesson learned from Billroth I and Billroth II was that bile reflux can be a significant problem when creating the continuity of the proximal GI track with exclusion of the pyloric valve. In Bilroth II, there is the additional burden of the bile flowing toward the stomach unlike the Billroth I.
The SADI or SIPS, Loop procedures that are incorrectly promoted as “duodenal switch” employ a loop anastomosis, which results in a biliary flow toward the post pyloric duodenum significantly increasing the chance and the possible incidence of Bile reflux.
All these unknowns about the SIPS, SADI Loop are yet to be investigated.