Category: Absorption
Osteoporosis Medications
March 28, 2020 7:22 pm
There are a number of lectures, posting that we have done over the years on this topic. However the questions of osteoporosis medications and their benefits and risks comes up often.
The links are attached:
Here is an updated list of medication that I had previously published. I made some clarification to explain how the medications work. There are different classes of medications and the detail of the action and soda effects were described earlier at a blog post.
List of medications that effect bone health.
The table is obtained from https://www.nof.org site.
Overfed But Undernourished
October 01, 2019 11:27 am
Obesity is related to as many as 400,000 deaths each year in the US and it has increasingly been recognized as a risk factor for several nutrient deficiencies. This may seem surprising given the likelihood of over consumption of calories, however these additional calories are not from nutritious sources. One of the main reason for these nutritional deficits is the greater availability of inexpensive foods that are rich in calories and are nutrient deficient. This has led some medical professional to conclude that there is a certain group of people who are overfed but undernourished. Even with the epidemic of the obesity, there is significant nutritional deficiencies noted.
Obese subjects have increased blood volume, cardiac output, adiposity, lean mass and organ size all of which can influence volume of distribution, in addition, treatment for severe obesity involving surgical procedures can worsen these nutrient deficiencies and in some cases may cause new ones to develop.
This table shows the percentage of population below the estimated average requirement (EAR) by body weight status in adults more tan 19 years old, showing that almost 90 to 100 percent of people including normal weight (NW) are below the EAR of vitamin D and Vitamin E.

We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Vitamin A, Absorption, and Wound Healing
September 25, 2019 8:39 am
Vitamin A is one of the 4 fat soluble vitamins along with vitamin D, Vitamin E and Vitamin K. It is multifunctional and essential which means that it is not produced by the body. In this article we will touch on aspects of Vitamin A absorption and it’s effect on wound healing as well as its metabolism.
We often think of Vitamin A as the critical vitamin for vision, however it has several other roles that related to immune function, protein synthesis, and cellular communication. Vitamin A deficiency is a concern world wide because of the natural of the side effects. Vitamin A deficiency is the leading cause of preventable childhood blindness in the world according to UNICEF and sometimes it may be undetected until there is irreversible damage.
There are 2 chemical forms of vitamin A in diet:
Retinoids (Preformed vitamin A) This group include retinol, retinyl esters, and retinal they are mostly found in animal sources like liver, egg yolk or fish oils.
Carotenoids (Provitamin A) This group includes beta-carotene, alpha-carotene and lycopene, mainly found in plant sources like leafy vegetables or yellow/orange vegetables and fruits.
The Physiology of the Vitamin A is as follows:
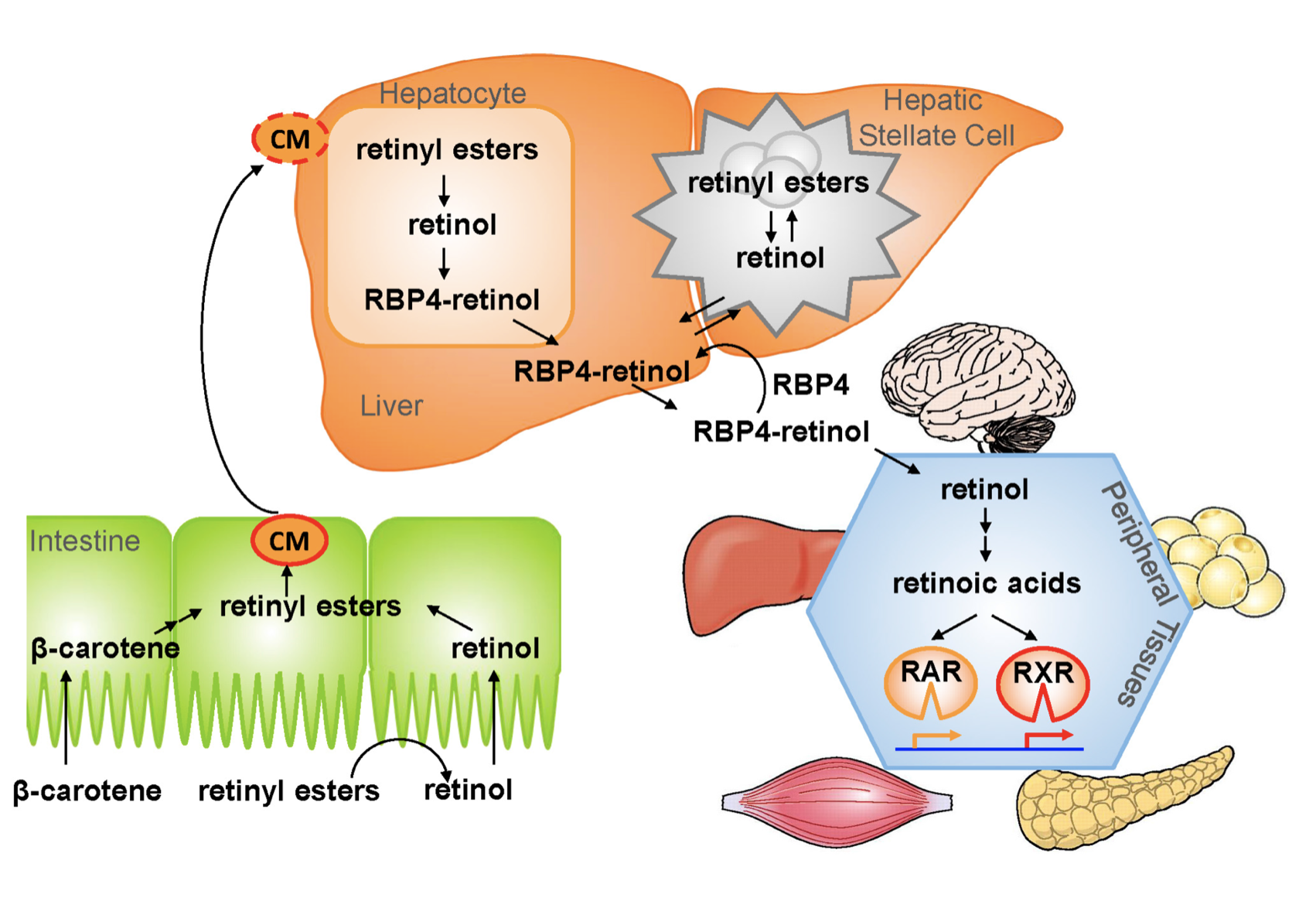
1.- Ingested food is digested in the stomach where retinyl palmitates (esters) are released from proteins. Retinol and beta-carotene are absorbed directly into the small intestine where retinyl esters and betacarotene are transformed into retinol . Retinol is the most easily absorbed form of vitamin A.
2.-That retinol absorbed by the enterocytes in the ileum (small intestine) along with bile is then transported to the liver with the help of chylomicrons a protein that transports fat.
3.-Fifty to 80% of the vitamin A is stored in the liver and the remaining is deposited into adipose tissue, lungs and kidneys.
4.-When stored retinol is released from the liver into the circulation to target organs, it is bound to plasma retinol-binding protein (RBP4) a transporting protein produced by the liver that requires ZINC, which is synthesized by the liver; This complex is stabilized by transthyretin (TTR), which reduces renal excretion.
Retinol is a crucial component for reproduction, embryological development, cellular differentiation, growth, protein synthesis, and immunity in the form of retinoic acid and vision in the form of retinal.
One of Vitamin A additional roles is in epithelial health of skin and mucous membranes. It increases epithelial turnover which is crucial during would healing. It also has anti-oxidative effects which prevent cell damage and can prevent or reverse the effects of other damaging agents. In addition to these benefits it has also been associated with increasing collagen, fibronectin, keratinocytes and fibroblast, all important in wound tissue structure. There have been some studies that suggest giving higher doses of Vitamin A in patients with non or slow healing wounds.
It is important to remember that we have documents delayed diagnosis of adult vitamin A deficiency leading to significant night blindness in adults. It is critical that the patients and their primary care physicians are acutely aware of this possibility. In majority of the patients with low vitamin A, post weight loss surgery, aggressive supplementations, including injections need to be considered as a part of the treatment regimen.
We would like to thank Miguel Rosado, MD for his significant contribution provided for this Blog.
Small Intestine
September 25, 2016 10:27 am
The small intestine is a long tubular organ that is approximately 460-1000cm in adults. It is divided into three sections, Duodenum, Jejunum, and Ileum. The surface area is greater than one might think due to the folds, villi, and microvilli. The surface area is approximately 30 square meters. Most of human digestion and absorption takes place within these three sections of small intestine.

The diagram of normal anatomy absorption in the small intestine is pictured to the right. It is color coded based on the area of the digestive tract the absorption takes place. You may also view here: master-normal-anatomy-with-text
Overview
Length: 22 ft. (6.7 m)
Width: 1 inch
pH: neutral or slightly alkaline (5-7)
- Steps:
- Neutralization in stomach, where enzymes act to breakdown food
- Digestion through greater breakdown with help of bile and pancreatic juices
- Absorption through assimilation of digested food, vitamins, and salts. Nutrients are taken into the bloodstream via specialized epithelial cells to the liver through the hepatic portal vein.
Duodenum
Length: 1 ft. (0.30 m)
pH~ 5
- Main site of breakdown
- C shaped turn with 4 parts: superior, descending, inferior, ascending
- Mixes food (now in form of chyme) with bile and other digestive juices
- Passes chyme through duodenojejunal flexure which contains suspensory muscle to widen the duodenal angle and increase movement.
Jejunum
Length: 8.2 ft. (2.5 m)
pH~ 6
- Coiled, vascular tube that contains a thick intestinal wall
- The wall contains epithelial projections called intestinal villi
- Smaller projections in the villi, called microvilli work to:
- project specialized transport cells called enterocytes
- increase surface area
- allow more absorption
Ileum
Length: 11.5 ft. (3.5 m)
pH~ 7
- Less vascularized and thinner intestinal wall
- Absorbs nutrients that preceding sections of the gut did not
- particularly works with vitamin B12 and bile salt absorption
- Connects to the colon through the ileocecal valve for further breakdown.
The following are Member Exclusive documents. Please be aware of your terms of use of these items.
Click for: [ddownload id=”7048″ style=”link” text=”Duodenal Switch Absorption & Anatomy (%filesize%)”]
Click for:[ddownload id=”7049″ style=”link” text=”RNY Absorption Anatomy (%filesize%)”]
References:
- Campbell NA, Reece JB, Mitchell LG. Biology. 5th ed. Benjamin-Cummings Pub Co. 1999-2002; 802-805.
- Ovesen L, Bendtsen F, Tage-Jensen U, Pedersen NT, Gram BR, Rube SJ. Intraluminal pH in the stomach, duodenum, and proximal jejunum in normal subjects and patients with exocrine pancreatic insufficiency. Gastroenterology. 1986; 90(4): 958-62.
- Stevens C. E., and Hume, I. D. 1995.Comparative Physiology of the Vertebrate Digestive System. 2nd ed. New York: Cambridge University Press.
- Schmidler C. Anatomy and Function of the Digestive System. Healthpages.org. 2016.
Metabolic Processes In Different TissuesExclusive Member Content
February 11, 2016 8:29 am
Hypertrophy of Small Bowel and Weight Gain Years After Duodenal Switch
August 21, 2015 7:53 pm
Duodenal switch (DS) operation results in the highest success rate of all weight loss surgical procedures. Patients, over time, will experience some weight gain many years after DS procedure. There are a number of suspected mechanisms that may be responsible for the weight gain:
1-Ageing may slow the metabolism and the activity down.
2-Over time patients may not be as adherent to healthy dietary and lifestyle changes as they may have been immediately after surgery.
3- Hypertrophy of the alimentary and common channels over time increases in surface area f allowing greater caloric absorption leading to increased weight gain.
It has been demonstrated in bowel resection studies, as well as rat studies, that the nutrient stimulated regions of small intestine increase villus height and total weight, crypt depth and proliferation as well as wall thickness, as an adaptation to compensate for the loss of absorptive capacity in the resected bowel. This observation may be applied to DS procedure as seen in histological slides from a patient who had to have an operation done requiring bowel resection. The segment of the bowel resected included the junction of the biliopancreatic, common and alimentary limbs.

Vitamin’s Physical State And Solubility are Two Different Things.
March 29, 2014 6:11 pm
Drug interactions and Herbal Supplements
September 25, 2002 8:03 pm